
Researchers in 2023 provided evidence-based guidelines for deciding how many embryos to transfer, as prepared by ESHRE.
These are official recommendations to help decide on the number of embryos to transfer by the European Society of Human Reproduction and Embryology (ESHRE), based on existing data up to 2023.
Common acronyms that will be used in this post are single embryo transfer (SET) and double embryo transfer (DET).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
The ESHRE guidelines cover a wide range of different factors to consider in choosing the number of embryos to transfer:
- The risk of multiple pregnancy
- Clinical factors (history of previous failed transfers, age, ovarian response, etc.)
- Embryo factors (cleavage stage vs blastocyst stage, fresh vs frozen, PGT-A, etc.)
- Other factors (fetal reduction, transferring more than 2 embryos)
- Patient counselling (not covered here)
It is a massive 100+ page document that summarizes key studies that ESHRE used to form their guidelines. I highly recommend you check it out in it’s entirety, and I’ll be referring to specific pages that contain useful charts. You can find the link to the pdf here.
In this post, I’ll cover some of ESHRE’s main points, along with some representative studies, and contrast it with what the American Society for Reproductive Medicine (ASRM) recommends from their 2021 guidelines (which I review here).
Spoiler alert — ESHRE recommends one embryo in all cases! Why this is has to do with the increased risk of a multiple pregnancy.
Why single embryo transfers?
ESHRE argues that a single embryo transfer is preferred for 3 reasons:
- Decreased risk of pregnancy and fetal complications
- Decreased costs
- Reduced psychological burden
Decreased risk of pregnancy and fetal complications
Eapen et al. (2020) did a meta-analysis to combine the results of 60 studies looking at maternal and fetal risks with a single pregnancy vs twins after IVF.
For maternal risks, they found:
- 3.7x increase in the odds of a Cesarean delivery
- 2.0x increase in the odds of pregnancy-induced hypertension
- 6.3x increase in the odds of preterm labor
- 1.9x increase in the odds of preeclampsia
For fetal risks, they found:
- 8.3x increase in the odds of a preterm birth
- 10.6x increase in the odds of a baby born with a low birthweight (<2,500 g)
- 6.5x increase in the odds of the baby being admitted to NICU/SCBU
- 2.2x increase in the odds of a stillbirth
They have a good chart that summarizes multiple studies on pg. 20 of the guidelines.
Decreased costs
Some studies show that a single embryo transfer can be a less costly option over a double embryo transfer, because of reduced risks of complications. This was demonstrated in multiple European countries, Canada, Japan and the US. Carpinello et al. (2016) found that delivery and neonatal procedures in the US for SETs resulted in a cost of $71,860, compared to $171,350 for DETs as a result of complications.
As far as I can tell, the data they list has more to do with costs relating to the healthcare system rather than the out-of-pocket costs for the patient.
In the US, many people have high deductible insurance plans, that ultimately absorb a lot of the cost once the deductible is reached (which is inevitable if you’re going to the hospital for a very expensive delivery). So if you’re going in the hospital for a delivery anyway, any added cost due to complications would be covered by the insurance, so I don’t think patients would have any additional out-of-pocket costs.
A more significant burden might be the repeated embryo transfers with an SET vs a DET, as these are often not covered by insurance in the US.
In countries where insurance covers IVF or transfers, there may be a limit on how many cycles the patient can do. So in these cases it might be make sense to do a DET instead of an SET, for certain patient groups.
Reduced psychological burden
ESHRE also presented research showing that having more than one child can lead to mental health problems such as depression and anxiety. These problems can last for years after childbirth, so support is important.
Factors like birth circumstances, emotional issues and the quality of the parents’ relationship can affect maternal mental health. Co-parenting can reduce stress, but moms of multiples may still feel more stressed.
Deciding on transferring 1 vs 2 embryos: Considering female age
ASRM’s 2021 recommendations are built around allowing older women to transfer more than one embryo, to compensate for reduced success rates with age.
Ma et al. (2022) performed a meta-analysis and combined the results of 85 studies (with only a few studies with women >40).
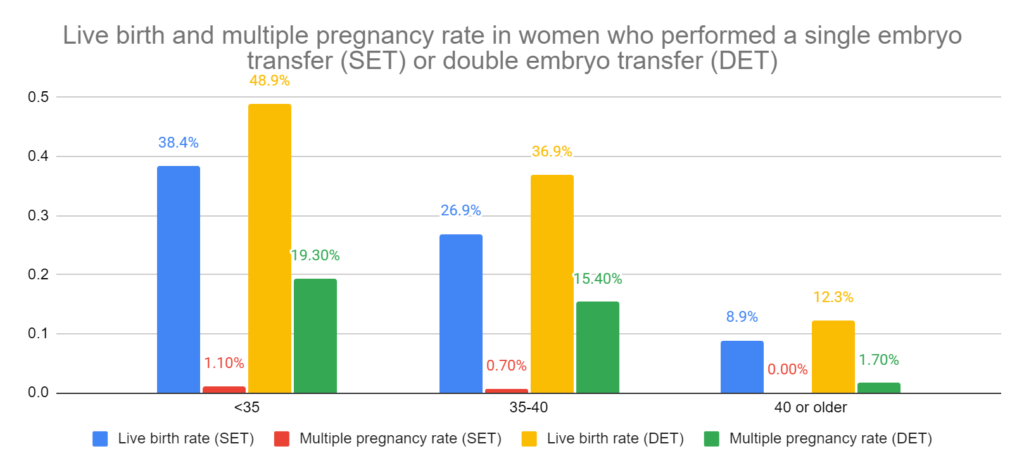
Compared to DET, SET lowered the odds of a live birth by 22% for all ages. When patients were grouped by age:
- For women <35, SET lowered the odds of live birth by 29%.
- For women 35-40, SET lowered it by by 20%.
- For women >40, there was no difference between an SET and DET. This means that having a SET or DET had the same chance of live birth in women >40.
Compared to DET, SET lowered the odds of a multiple pregnancy by 95% for all ages. When patients were grouped by age:
- For women <35, SET lowered the odds of a multiple pregnancy by 97%.
- For women 35-40, SET lowered it by 96%.
- For women >40, there was no difference between an SET and DET. This means that having a SET or DET had the same chance of multiple pregnancy in women >40.
Although it wasn’t mentioned, a possible reason they’re not seeing a difference for women >40 is because there isn’t much difference in the live birth rate after transferring one or two for women this age. ESHRE addresses transferring more than two embryos further along in the document (pg. 91), but there isn’t much data for older patients.
Some additional studies considered by ESHRE did find differences for DET in older patients.
A nice summary table that shows the outcomes for live birth rate (LBR), cumulative live birth rate (cLBR), multiple pregnancy rate (MPR) and more can be found on pg. 49.
Overall, ESHRE recommends a single embryo transfer for women of all ages. This is true even for older women, who are at an even greater risk of pregnancy and fetal complications that are exacerbated with a multiple pregnancy.
In contrast to these recommendations, ASRM allows more embryos to be transferred with advancing age due to the lower success rates with age. It’s a shame there isn’t more data on this to see what impact transferring an increasing number of embryos has on live birth and multiple pregnancy rates.
Deciding on transferring 1 vs 2 embryos: Considering embryo quality
Patients often base their decision to transfer one or two embryos on the quality of the embryo. If they have good quality embryos, they might only transfer one, but if they have poor quality embryos, they might want to transfer two to make up for the reduced success rates. Some patients also like to add a poor quality embryo along with a good quality one when transferring.
ESHRE looked at a bunch of studies that cover this, either with cleavage stage or blastocyst stage transfers, that were fresh or frozen.
Cleavage stage embryos
There are quite a few studies laid out by ESHRE (along with some RCTs!), but let’s look at the results of Zhu et al. (2020), who used frozen embryos that were good quality or poor quality. There was a pretty even mix of patients across all ages in this study, with nearly 25,000 cleavage stage transfers. Good quality embryos had 4 cells on day 2 or 6-8 cells on day 3, with <20% fragmentation.
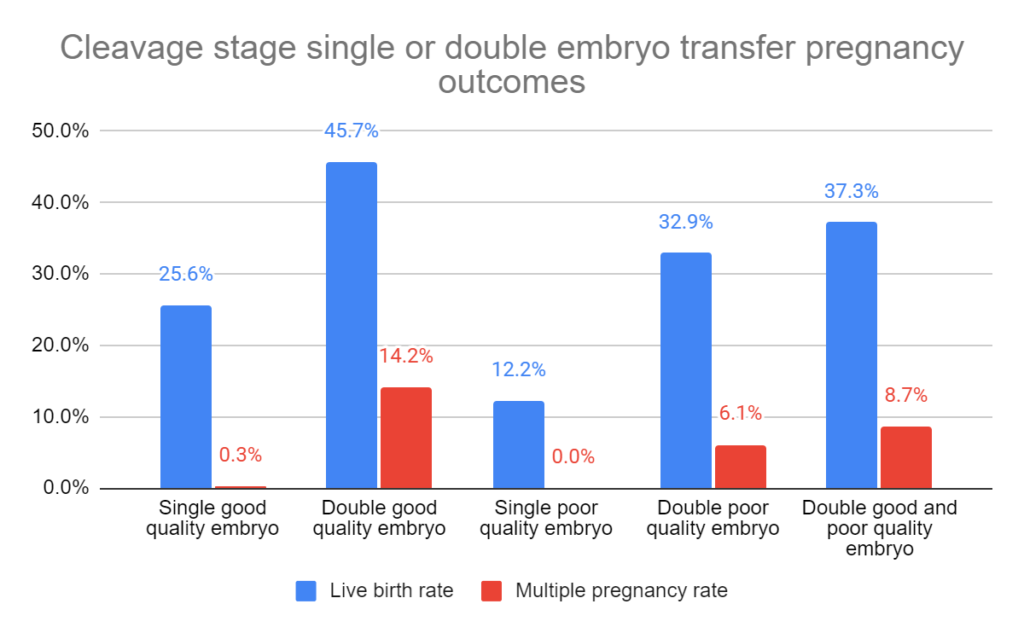
For live birth rates, when they statistically adjusted these results to control for differences between the groups (like age):
- Odds of a live birth were half with one poor quality embryo vs one good quality
- Odds were 62% higher with 2 good quality embryos vs one
- Odds were 25% higher with a good and poor quality embryo vs one good quality
- No difference for 2 poor quality embryos vs one good quality. This means that transferring 2 poor quality embryos was equivalent to transferring 1 good quality embryo — for live birth rates only! Note that there is an increase in the risk of multiples!
For fresh cleavage stage SET or DET involving good quality embryos (GQE), poor quality embryos (PQE) and mixed quality embryos (MQE), refer to the chart on pg. 68. For frozen embryos, see pg. 80. These charts lay out all the studies that ESHRE considered, with some studies finding a difference for SET and DET, while others didn’t.
Blastocyst stage
Again, ESHRE outlined many studies relating to fresh/frozen blastocysts. I’ll just show the results of the Zhu et al. (2020) study, which did a good job of grouping good/poor quality embryos. There was a pretty even mix of all ages, with about 2,000 patients doing blastocyst transfers. Good quality embryos were 3BB or higher.
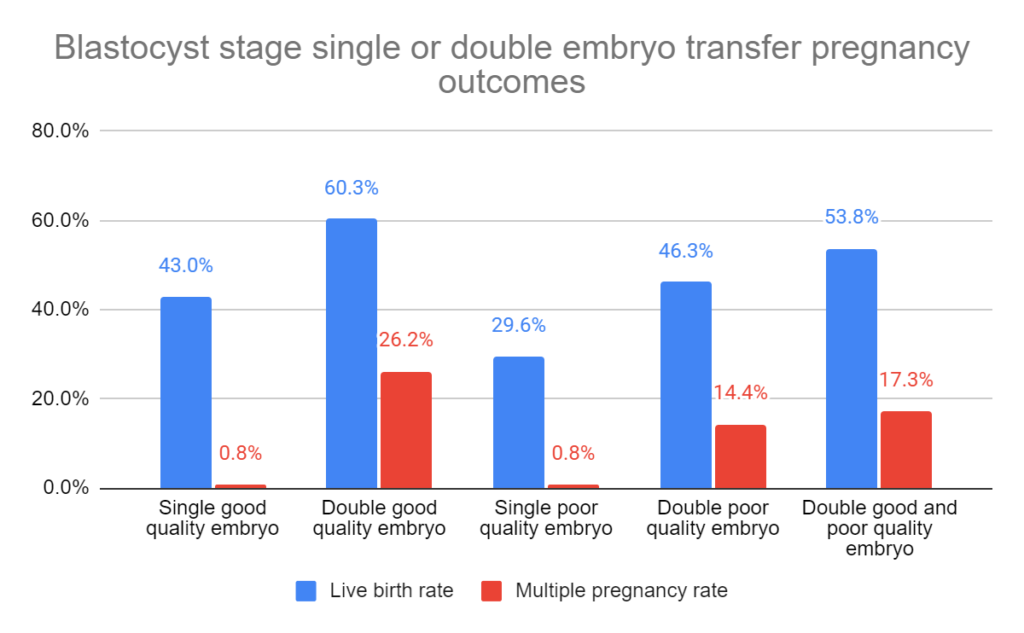
For live birth rates, when they statistically adjusted these results to control for differences between the groups (like age):
- Odds of a live birth were 38% lower with one poor quality embryo vs one good quality
- Odds were 76% higher with 2 good quality embryos vs one
- No difference with a good and poor quality embryo vs one good quality. This shows that including a poor quality embryo had no further benefit on live birth rates, although it did increase the risk of multiples!
- No difference for 2 poor quality embryos vs one good quality.
For fresh blastocyst stage SET or DET involving good quality embryos (GQE), poor quality embryos (PQE) and mixed quality embryos (MQE), refer to the chart on pg. 73. For frozen embryos, see pg. 85. These charts lay out all the studies that ESHRE considered, with some studies finding a difference for SET and DET, while others didn’t.
ESHRE’s recommendation
Based on the available evidence, they recommend a single cleavage stage or blastocyst stage embryo can be transferred. Most of the studies they looked at compared good quality SETs and DETs. In some cases, there were no differences between live birth rates — but there was always an increase in the multiple pregnancy rate.
Deciding on transferring 1 vs 2 embryos: Other factors
History of failed transfers. The ASRM allows patients with previous failed transfers (using high quality embryos) to consider an additional embryo. ESHRE found no evidence to support this position and they recommend SET.
How long a patient has been infertile. ESHRE found no studies were found that specifically compare SET and DET in patients who had been infertile for different lengths of time. SET is recommended.
Ovarian response. SET is recommended.
Endometrial factors. SET is recommended, regardless of endometrial thickness, morphology or other measures.
Donor eggs or embryos. SET is recommended.
Gestational carriers. SET is recommended.
Time-lapse embryos. SET is recommended.
PGT-A. There’s no studies that look at double embryo transfers using low mosaic, segmental, etc. embryos. SET is recommended.
Fetal reduction. Fetal reduction can be considered to reduce complications. The procedure itself has risks, so SET should be prioritized.
Conclusions
ESHRE recommended a single embryo transfer in every situation they covered in their guide, as it relates to:
- Maternal age
- Embryo quality
- History of failed transfers
- Infertility duration
- Ovarian response
- Endometrial factors
- Use of donor eggs/embryos
- Gestational carriers
- Time-lapse embryos
- PGT-A
The reason they only recommend one is because there’s an increased risk of complications for both the mother and baby when transferring two embryos.
Based on the studies they covered, the chance of a live birth didn’t always increase with a DET vs a SET, but the chance of multiples always increased.
In my opinion, while it’s clear that SETs are ideal for all patients to reduce the risk of complications, it may not be realistic when considering the additional time and expense.
A single embryo transfer for patients in their 40s has a low chance of success, requiring numerous transfers. In the US, these procedures may not be covered, so transferring multiple embryos would likely help to minimize expenses and reduce time-to-pregnancy. The ASRM, which is based in the US, recommends a higher number of embryos to be transferred with advancing age, which may be a reflection of the healthcare situation in the US. Even in other countries, patients may be limited in how many cycles are covered by the government.
It’s a shame that there isn’t more data on multiple embryo transfers in older patients, to better understand how this affects live birth and multiple pregnancy rates. ESHRE might recommend more than one embryo in these patients if there was more data available.
Regardless, it’s important to discuss the number of embryos transferred with your doctor and ESHRE provides a great overview of the available data to help make those decisions.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 2 embryos or 1? The risks of a double embryo transfer for women under 35
2 embryos or 1? The risks of a double embryo transfer for women under 35
 How many embryos to transfer? 2021 ASRM recommendations
How many embryos to transfer? 2021 ASRM recommendations
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Researchers examine factors associated with preterm birth risk in IVF
Researchers examine factors associated with preterm birth risk in IVF
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 Study explores if transferring two embryos puts one at risk
Study explores if transferring two embryos puts one at risk
 Can one embryo split to become triplets? Rare IVF cases after single embryo transfer
Can one embryo split to become triplets? Rare IVF cases after single embryo transfer