NK or natural killer cells play an important (and controversial) role in IVF. Most evidence suggests that there is no link to NK cell levels and pregnancy outcomes, and that immunotherapies that target NK cells in IVF show no benefit. Although there may be a certain group of patients that benefit. We’ll also discuss how uterine NK cells can support pregnancy, with information on their KIR receptors and HLA-C on the embryo, and how this can lead to embryo “rejection.” Finally, we’ll look at the overall problems with NK cell testing.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
What are NK cells?
The immune system’s job is to identify and eliminate potential threats to the body, and to do this it uses multiple cells. One of these cells is the natural killer (NK) cell, as shown below.
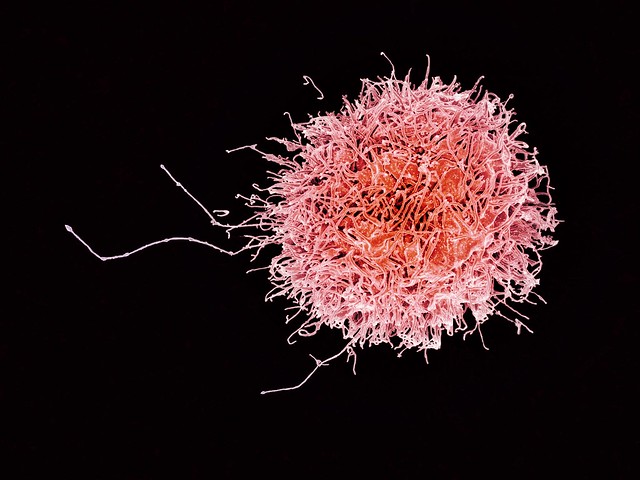
NK cells usually target virus infected cells or tumor cells. Tumor cells actually form naturally in our body and NK cells eliminate them before they get out of hand and become cancer.
There’s all kinds of different NK cells. There’s NK cells in the lungs, in fat, in the brain…they’re all over the place! Our body is made up of multiple tissues and the immune system has adapted to make specialized immune cells for those tissues.
So it’s no surprise that NK cells also have a place in the uterine environment and implantation.
What kind of NK cells are involved in implantation?
When it comes to NK cells in IVF, we usually are talking about two types:
- The peripheral blood NK cells (pbNK cells) – these are NK cells that are in the blood
- The uterine NK cells (uNK cells) – these are in the uterus
The pbNK cells act like killers indeed! They’ll target and kill foreign threats to the body. They do this because the blood can be a vulnerable space for infection.
In the uterus, there’s less risk of exposure to infection and the uNK cells have a different behavior. They don’t participate in killing cells, and instead play more of a supportive role for embryo implantation (Moffett et al. 2015):
- Help build blood vessels for implantation and formation of the placenta
- Promote embryo invasion into the endometrium
There are different types of uNK cells, which are classified based on how much CD56 they have on their cell surface. CD56 is a type of cell surface protein that scientists use to identify these cells. NK cells that have a lot of CD56 are called “super bright” because of how strong the signal is using lab instruments to measure them. “Dim” NK cells don’t have much CD56.
There are two types of uNK cells – the “super bright” and “dim” varieties. About 90% of the uNK cells are super bright, and 10% are dim. This might be an important ratio and may be different in women with recurrent miscarriage (Sacks 2015).
How do uNK support pregnancy?
In this section we’ll discuss more about how uNK cells can support a pregnancy when they’re activated, and how they can “reject” a pregnancy when they’re inhibited.
In general, an activated uNK cell means that it produces factors that support implantation and formation of the placenta, while an inhibited one doesn’t produce these factors. Inhibited uNK cells could lead to implantation failure or a miscarriage.
Note that this information mostly came from Wasilewska et al. (2024). I’m simplifying a lot of this to make it easier to understand, feel free to check out the original paper to get more details (it’s open access).
KIR receptors and HLA-C
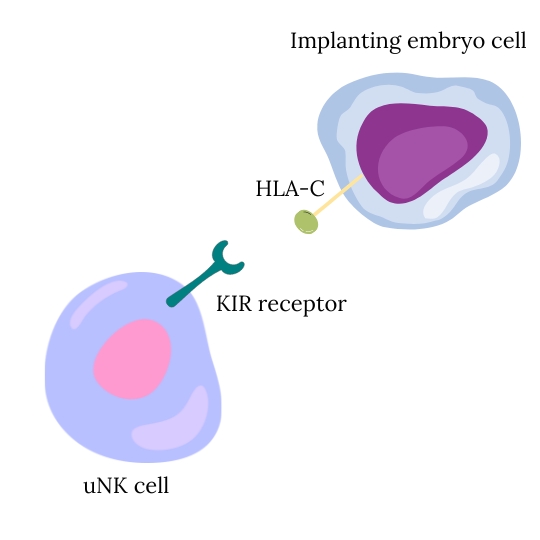
There are certain molecules on the surface of the NK cell and the implanting embryo that can bind together to activate or inhibit NK cells. Certain combinations seem to work better for implantation.
What are these molecules called?
- On NK cells, these are called Killer cell immunoglobulin-like receptors, or KIR receptors.
- On the implanting embryos, these molecules are called human leukocyte antigen or HLA. There are many different types of HLA, and the one we’ll talk about is HLA-C.
Extra information: HLA (also known as MHC when not talking about humans) are a group of genes that code for special proteins that can be presented on the surface of our cells. These HLA proteins can combine with other proteins that our body makes to calibrate our immune system to recognize itself and not attack our own cells. HLA is what determines donor compatibility during organ transplants!
Extra information part 2: The “implanting embryo cell” is called an extravillous trophoblast or EVT. These cells are derived from the trophectoderm of the blastocyst that have the job of invading into the endometrium to start remodeling blood vessels to form the placenta. EVTs form after the embryo implants.
KIR receptors and HLA-C combinations affect implantation
There’s a lot of variability in the KIR receptors and HLA-C molecules between people, and different studies have looked at how they can affect implantation.
KIR receptors can be activating or inhibitory and can be broken up into haplotype A and B (a haplotype is a group of genes that are inherited together). Haplotype A mostly consists of inhibitory KIR receptors, while haplotype B mostly consists of activating KIR receptors.
Activating and inhibitory in this sense means that once the receptor binds to its HLA-C, it either activates the uNK cell or inhibits it. Activated uNK cells produce beneficial factors for implantation.
Humans have two copies of each gene (ie. they’re diploid), and they can inherit two KIR haplotypes:
- Those with two copies of the KIR A haplotype (KIR AA) will mostly have inhibitory KIR receptors.
- KIR BB individuals will mostly have activating KIR receptors.
- KIR AB individuals will have a mix.
For HLA-C, there’s 2 types called C1 and C2, with different types of C1 and C2. HLA-C2 strongly binds with inhibitory KIR A receptors.
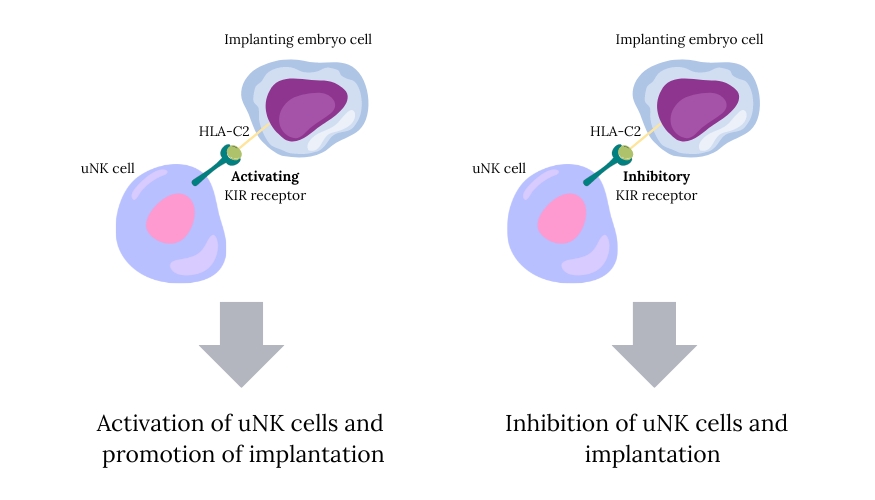
Women with KIR AA whose embryo has HLA-C2 are at increased risk of recurrent implantation failure. This is because the KIR A receptors on the uNK cells are inhibitory, and when they bind to HLA-C2 on the implanting embryo this causes inhibition of the uNK cells, so they don’t produce beneficial factors for implantation.
However, the opposite happens in women with KIR B receptors. These receptors bind to HLA-C2 and this activates the uNK cells, so they produce beneficial factors for implantation.
In reality, it’s much more complicated than this, because there are multiple receptors involved. The KIR A haplotype actually consists of 5 receptors: KID3DL3, KIR3DL2, KIR3DP1 and KIR2DL4 are all inhibitory; and KIR2DS4 which is activating. So if someone inherits KIR AA then they’ll have these 5 receptors scattered on their uNK cells, all of which have variable binding potential to the HLA-C molecules on the implanting embryo.
The actual KIR receptors present are also variable between people, so two people with a KIR A haplotype will have the same general receptors, but they’ll be slightly different (ie. there are different alleles). As of early 2024, there’s about 2,200 KIR alleles that have been identified (https://www.ebi.ac.uk/ipd/kir/alleles/).
There’s also two major types of HLA-C called HLA-C1 and HLA-C2, which together consist of about 20 different forms (alleles). Two of these will be inherited: one from the mother and one from the father, so the embryo will carry two types of HLA-C.
All of these HLA-C molecules have a different affinity for all the different KIR receptors, where some will be activating and some will be inhibiting. Ultimately, the combination of all these signals is what dictates whether implantation will be supported or not. Because of all the variability, this leads to a highly individualized response to an implanting embryo.
So am I compatible with my partner?
With all these different combinations of KIR receptors and HLA-C, we can see that some are more compatible than others.
Couples can be genotyped by testing their DNA to see if they carry compatible KIR and HLA-C versions.
As mentioned in the previous section, women with KIR AA with an embryo that has HLA-C2 tend to have an increased risk of implantation failure. The KIR AA genotype is determined in the mother, while the HLA-C2 genotype from the embryo would need to be assessed from both the mother and father.
Can NK cells cause pregnancy loss?
When most people talk about NK cells in IVF, they’re usually referring to pbNK cells from the blood (not what’s in the uterus). This has created a lot of controversy because uNK cells are in the uterus and have a supportive role. pbNK cells are generally not in the uterus, although it’s possible that pbNK cells can migrate into the uterus and turn into uNK cells (Carlino et al. 2008).
So why do we care at all about pbNK cells?
In 1995, women with reproductive failure were tested for NK cells for the first time. Beer et al. (1996) made the observation that there were elevated levels of these cells in the blood of women with reproductive failure.
The author of this paper published a book based on this observation, “Is your body baby ready?“, which attributed NK cells as the cause for some cases of reproductive failure. It’s been criticized as a case of “blatant opportunism” and being premature in making such a strong conclusion based on “poor quality observational studies” (Sacks 2015).
Just because there’s an increase in NK cells with reproductive failure, doesn’t mean that NK cells cause reproductive failure. Correlation doesn’t equal causation. For example, when ice cream sales increase, so do drownings. This is because of the warmer weather during the summer, which causes people buy more ice cream and go swimming. It’s not the ice cream that causes drownings, it’s the warmer weather. You wouldn’t try to stop drownings by restricting ice cream sales.
This is the problem with basing conclusions on observational data.
The majority of NK cell and IVF data is observational and shows levels of NK cells can vary with infertility. A meta-analysis by Seshadri et al. (2013) summarized 22 research papers on pbNK and uNK cell numbers as it relates to infertility and found:
- No difference in pbNK/uNK cell % in infertile women vs controls
- Higher % of pbNK cells in women with recurrent miscarriage vs controls
- Higher number of pbNK cells in infertile/recurrent miscarriage vs controls
- No difference in % of uNK in women with recurrent miscarriage vs controls
- No difference in live birth rates in women with high pbNK levels/activity
This shows that some groups of women might have increased levels of pbNK cells. Whether or not this is causing their infertility isn’t addressed.
A more recent meta-analysis by Von Woon et al. (2022) combined 60 studies that looked at NK cells in women with recurrent implantation failure (RIF) or recurrent pregnancy loss (RPL), and found:
- Higher levels of uNK cells in women with RIF.
- No difference in pregnancy outcomes in RIF/RPL women based on uNK cell levels.
- No association with pbNK and uNK cell levels in women with RIF/RPL.
- There was too much variability in the studies to draw conclusions on uNK cell activity.
Based on these last two meta-analyses, higher levels of pbNK and uNK cells may be associated with infertility. However, this their levels aren’t associated with differences in pregnancy outcomes, and the data is too variable to draw conclusions based on their activity.
NK cell treatment
Immunotherapies can be used to suppress the immune system, including intralipids, IVIG, and prednisone. These drugs suppress not only NK cells, but much of the immune system in general, although most patients take these drugs to suppress NK cells.
A recent meta-analysis by Melo et al. (2022) combined studies in patients who mostly had implantation failure and found:
- No change in live birth rate with aspirin (6 studies).
- No change in live birth rate with heparin (3 studies).
- No change in live birth rate with corticosteroids (like prednisone) (5 studies).
- Increased live birth rates with G-CSF (5 studies).
- No change in live birth rates with intralipids (2 studies).
- No change in live birth rates with IVIG (2 study).
- Decrease in live birth rates with hLIF (1 study).
- Increase in live birth rates with PBMCs (2 studies).
I review this study in detail in my post Meta-analysis of commonly used IVF immunotherapies shows no benefit.
Another recent randomized controlled trial (RCT) by Sun et al. (2023) found no benefit for RIF patients who used prednisone. I reviewed this study here.
If there isn’t much good quality evidence for treating NK cells, why are people seeking this treatment?
This is because it seems to work for some people, and clinics will do their best to provide treatments that patients want (otherwise they’ll go elsewhere!).
So I can think of two reasons why these treatments are working:
- Having another transfer would have worked anyway, regardless of the immunotherapy.
- It really does work.
So who is benefiting? It’s possible that there’s a group of people with an undiagnosed immune disorder that causes their infertility.
The issue is we don’t know who these people are, so researchers can’t design studies to see if these treatments work on them. The best they can do is test these treatments in patients who have general infertility, or those with RIF or RPL, and see if there’s any difference. So far the evidence suggests that these groups don’t benefit, but this could change as more information comes out.
The problem with NK cell testing
The major problem with NK cell testing is that there is no consensus. What’s a “bad” level of NK cells? That changes depending on who you’re talking to, or what study you’re looking at.
Imagine playing baseball with different rules depending on who you played with. Having a consensus for the rules of baseball is important!
With no baseline on what’s normal vs abnormal, interpreting NK cell results can be very ambiguous. Moffett et al. 2015 warns that NK cell test results can have a high rate of “abnormal” results which are not credible.
Additional problems with NK cell testing are (Sacks 2015, Von Woon et al. 2022):
- Simple measurement of the uNK cell numbers tells us nothing about their activity.
- Cell numbers can change dramatically during a menstrual cycle (changing from 5 to 40% within 10 days) and there is no defined reference point for measuring these cells.
- The method of counting these cells isn’t consistent (some use IHC, others use flow cytometry).
- The markers used for NK cells may not be reliable in identifying NK cells from other immune cells.
- Many other immune cells are present in the endometrium, and these should be investigated also.
Other factors besides NK cells could influence implantation failure, and patients should consider these also (embryo aneuploidy, endometritis, uterine abnormalities, etc.). For a more comprehensive list check this post.
A final point I’ll make is that the use of immunotherapies targets a wide range of immune cells, and not just NK cells. It’s possible that altering these levels with immunotherapies could have a detrimental effect on pregnancy outcomes. A recent study found that, in general, higher levels of immune cells protect from miscarriage (reviewed here).
More studies are needed to better understand the role of the immune system in pregnancy, and “until then, measurement of uNK and administration of immunotherapy should be exclusively performed in research settings,” writes Von Woon et al. 2022.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 The impact of the vaginal and endometrial microbiome on reproductive health and IVF outcomes
The impact of the vaginal and endometrial microbiome on reproductive health and IVF outcomes
 Increases in immune cells associated with reduced risk of miscarriage
Increases in immune cells associated with reduced risk of miscarriage
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Shipping embryos or gametes to another clinic
Shipping embryos or gametes to another clinic
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer