The Preimplantation Genetic Diagnosis International Society (PGDIS), an organization of PGT-A experts, has published their 2021 guidelines for mosaic embryo transfers. This replaces their 2019 guidelines.
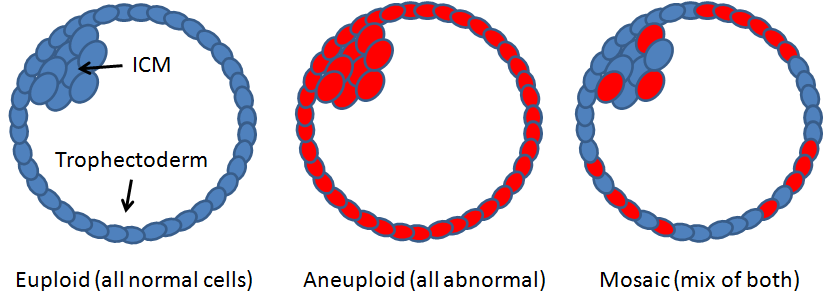
Mosaic embryos contain a mix of euploid and aneuploid cells and have an intermediate success rates. They represent about 5-15% of tested embryos, which seems to be variable between clinics.
Check my complete guide to mosaic embryos to learn more about mosaics, or my complete guide to PGT-A to get more background on PGT-A (aka PGS testing).
Different studies have shown a benefit for mosaic embryo transfers. Capalbo et al. (2021) (summarized here) found no difference between low level (<50%) mosaic and euploid embryos, while other studies, including Viotti et al. (2021) (summarized here), found that low level mosaics had a lower success rate compared to euploids. Low level mosaics have better success rates compared to high level mosaics.
There have been few cases where a mosaic embryo has led to the birth of a child with the associated abnormality. Mounts et al. (2019) reported the birth of a child with the segmental abnormality 15q11.2-q13, which was initially detected as a euploid but later re-examined and found to carry the segmental mutation as a 57% mosaic that was likely inherited from the father. In another case, Kahraman et al. (2020) reported on the birth of a child with 2% mosaicism of monosomy 2 after transfer of a 35% monosomy 2 mosaic.
So the risk of having a child with a specific abnormality from a mosaic embryo seems to be rare. However there may be reduced live birth rates, and increased miscarriage rates compared to euploid transfers.
Let’s go over some of the highlights of the recommendations that the PGDIS has made in their 2021 guidelines.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Recommendations for the PGT-A testing lab
- Thresholds <20% mosaicism = euploid, >80% = aneuploid.
- Avoid classifying mosaics as aneuploid, even with multiple affected chromosomes.
- Avoid labeling mosaics as “not suitable for transfer.”
- Lab reports should show % mosaicism, euploid threshold, and detected abnormalities.
Recommendations for the embryology lab
- Limit biopsies to 5-10 cells to protect the embryo from harm.
- Be cautious during biopsy and cell washing to prevent cell damage, as it may lead to higher mosaicism levels,
- Investigate the protocol or technique if consistently high mosaicism levels are reported.
Recommendations for genetic counsellors or support groups
- A single biopsy may not reflect the entire embryo, which could be mosaic even if it’s labeled euploid or aneuploid.
- The risk of a mosaic embryo resulting in a birth with the same abnormality is low.
- While higher % mosaic is linked to lower success rates, there’s no set cut-off for transfer eligibility.
- Many mosaic embryos were transferred without diagnosis before PGT-A.
Recommendations for the clinician
- PGT-A results aren’t always 100% accurate in diagnosing an embryo’s chromosomal status, so patients should be informed.
- Consent forms should mention the potential for mosaic embryos.
- In general, prioritize euploid embryos over mosaics.
- Inform patients that mosaic embryos may have a higher risk of negative outcomes, like miscarriage, and suggest additional PGT-A cycles to obtain euploids.
- Recommend prenatal testing for all IVF cases, regardless of PGT-A use.
Prenatal testing
- Recommend prenatal testing for all pregnancies post PGT-A or IVF.
- Use a 24-chromosome non-invasive prenatal testing (NIPT) method that covers the specific mosaic chromosome.
- Note that NIPT may not detect certain segmental abnormalities.
- NIPT assesses placental tissue, which can differ from the fetus’s chromosomal status.
- For the most definitive fetal status, consider invasive testing like amniocentesis after 14 weeks.
Recommendations for prioritizing mosaic embryo transfers
- High-level mosaics may have more negative outcomes compared to low-level ones, but we have limited data.
- Mosaicism percentage seems to be a better predictor of success than the affected chromosome.
- When % mosaicism is similar, consider the embryo’s grade, and prioritize whole chromosome mosaic embryos, followed by segmental aneuploids, and then segmental mosaics. After discussion with the corresponding author, this choice was a conservative one based on established data at the time of review. Newer studies will be covered in their next review.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to PGT-A (PGS testing)
Complete guide to PGT-A (PGS testing)
 Complete guide to mosaic embryos
Complete guide to mosaic embryos
 Ranking 1,000 mosaic embryo transfers
Ranking 1,000 mosaic embryo transfers
 Depletion of aneuploid cells in mosaic embryos
Depletion of aneuploid cells in mosaic embryos
 No difference in euploid and mosaic embryo transfers: a clinical trial
No difference in euploid and mosaic embryo transfers: a clinical trial
 Trophectoderm and ICM biopsies match depending on the abnormality
Trophectoderm and ICM biopsies match depending on the abnormality
 144 “abnormal” (aneuploid/mosaic) embryos and their outcomes
144 “abnormal” (aneuploid/mosaic) embryos and their outcomes
 Segmental aneuploids: the main source for PGT-A false positives?
Segmental aneuploids: the main source for PGT-A false positives?