This post covers mosaic embryos, including their definition, frequency after PGT-A, mosaic embryo levels (low level, high level), mosaic embryo types (whole chromosome, segmental), current guidelines for transfer, potential for self-correction, and success rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
What is a mosaic embryo?
Embryos, or cells, with the right number of chromosomes are called euploid and are considered normal. The “right number” of chromosomes is 46, and most of our cells have 46 chromosomes (except our sex cells). The 46 comes from 2 sets of 23 chromosomes (one set from the egg and the other set from the sperm):

An aneuploid embryo, or cell, has a different number of chromosomes (not 46).
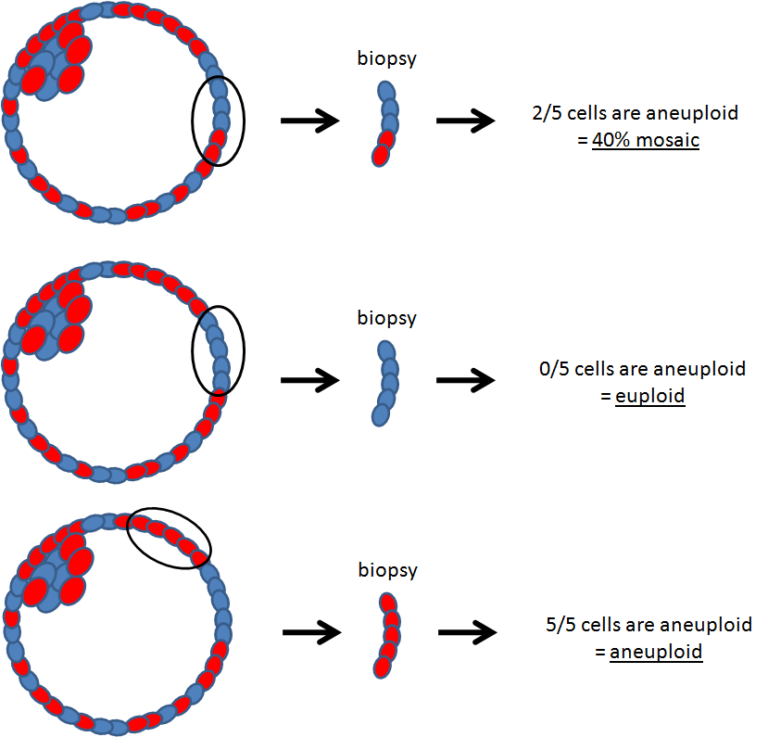
Mosaic embryos contain a mix of euploid (normal) and aneuploid (abnormal) cells as shown below:

Embryos that are totally aneuploid are due to errors in the egg or sperm (meiotic) that are carried over to every cell in the embryo. In mosaic embryos, an error occurs after fertilization (mitotic) and after the first cell starts dividing. Only the cells that divide from this one particular cell are affected.

It’s not clear what causes them. One possibility is that mosaics are the result of speedy cell division and relaxed “checkpoints” common in the embryo’s early growth, and these errors may be corrected afterwards (McCoy 2017). The embryo might correct itself through a variety of mechanisms as we’ll see.
Mosaic embryo levels (low level, high level)
To determine if an embryo is euploid or aneuploid, you can use a test called preimplantation genetic testing for aneuploidy, or PGT-A. This test involves taking a biopsy of an embryo and extracting the chromosomes (DNA) from the cells.
This DNA is sequenced and you can tell how many chromosomes there are, and whether or not the biopsy is euploid, aneuploid or mosaic. The results from the biopsy are assumed to be representative of the whole embryo.
For more background information, see my complete guide to PGT-A.
As sequencing technology improved (next-generation sequencing, or NGS), PGT-A gained better “resolution,” meaning it can detect smaller differences.
For example, in a biopsy of about 5 cells:
- If all 5 cells are normal → euploid
- If 1 out of 5 cells is abnormal → ~20% mosaic
Older methods couldn’t reliably detect this difference, but NGS can.
However, the technology still has limits. Differences below ~20% abnormal cells are difficult to detect, so lower levels of mosaicism may not be reported.
Mosaic embryos can be grouped based on the percentage of abnormal cells present:
- <20% abnormal (aneuploid) cells = euploid
- 20-40% = low level mosaic
- 40-80% = high level mosaic
- >80% = aneuploid
These thresholds are commonly used, but not universal. Some labs use different cutoffs, and recent guidance (ESHRE 2022) suggests grouping mosaics more simply as:
- <50% → low level
- >50% → high level
Always check your specific PGT-A report to see how your lab defines these categories.
How to read mosaic embryo PGT-A results
Your PGT-A report will show mosaic results using terms like “mos”, along with the affected chromosome and percentage. For example:
- mos(+2) 40% or +2 mos (40%)
This means that 40% of the cells in the biopsy are abnormal, with an extra copy of chromosome 2. If 5 cells were tested, this would be about 2 abnormal cells and 3 normal cells.
Whole chromosome vs segmental mosaics
There are two main types of mosaic abnormalities: whole chromosome or segmental.
In a whole chromosome abnormality, there’s a whole extra chromosome
- Whole chromosome additions (aka duplications) can be indicated as a “+” on a PGT report. Example: mos (+2) means there’s an extra copy of chromosome 2.
- Whole chromosome deletions can be indicated as a “-” on a PGT-A report. Example: mos(-3) would be a missing copy of chromosome 3.
- Note: Remember, there’s 2 copies normally. So a duplication would now have 3 copies in total, and a deletion would have 1 copy in total.
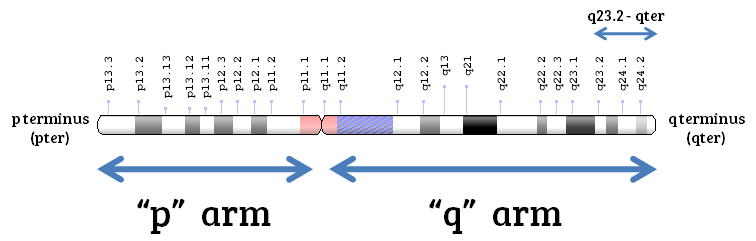
In a segmental abnormality, a segment or part of a chromosome is missing or duplicated.
- On a PGT-A report, this can look something like (q23.2-qter), which is referring to the specific positions of the deletion or addition on a particular chromosome.
- Chromosomes have two “arms” called the p arm and the q arm, and there are markers along each arm to specify particular locations, as you can see below:
Complex vs chaotic mosaics
It’s possible to have more than one chromosome affected in an embryo.
- Complex mosaics refer to mosaics with 3 or more chromosomal abnormalities.
- Chaotic mosaics refer to mosaics with 6 or more chromosomal abnormalities.
These definitions can vary so it’s important to check with your PGT report.
For more detail on reading PGT-A reports, see my complete guide to PGT-A.
How often do mosaics occur?
Based on standard PGT-A results
Capalbo et al. (2021) evaluated 6,766 PGT-A biopsies using NGS and found that mosaics occur at a frequency of 18.7%, with 12.3% being low level (20-30% aneuploid cells), 4.8% being moderate level (30-50%) and 1.6% being high level (50-70%).
The same study found that 58.1% were aneuploid (>70%) and 23.2% were euploid (<20%). The average female age was 38.

The above is a single study, and the incidence of mosaic embryos can be different depending on the clinic. Leigh et al. (2022) indicate that the mosaic embryos can range from 2-40%, but around 15% is commonly stated.
Armstrong et al. (2023) took this a step further and measured the chance of high and low level mosaics by age. Generally, they found that low level mosaics occurred at a frequency of about 3-10%, and high level mosaics at 5-9%.
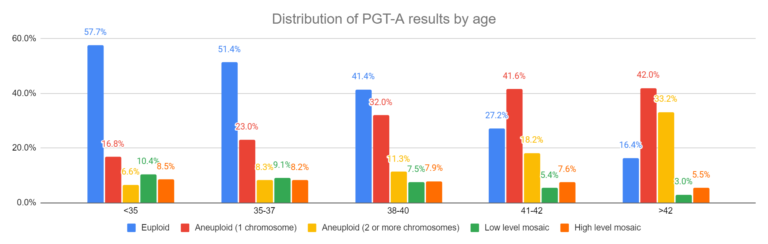
Read more in my post: A look at how PGT-A results change with age, using data from over 86,000 biopsies.
What more sensitive methods suggest
The above results are based on standard PGT — but what if a more sensitive test is used?
- Chavli et al. (2024) used single cell sequencing to check the chromosomes for each cell in an embryo, not just a single biopsy. They found that 82% of embryos have some extent of mosaicism. This is a very sensitive technique that can measure mosaicism much less than the 20% cutoff described earlier. Read more in my post Mosaicism much more common than previously thought, using more sensitive PGT-A technique.
- Zhai et al. (2024) used single-cell sequencing to analyze embryos and fetal tissues, finding that mosaicism is present in nearly all samples, suggesting that mosaicism is much more common than detected by standard PGT-A. Read more in my post: More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic.
- Yang et al. (2024) used a mathematical model to simulate embryo biopsies, finding that fully euploid embryos are rare and that most embryos are likely mosaic to some degree. Read more in my post: Mathematical model predicts that fully euploid embryos are rare.
Together, these studies suggest that mosaicism may be common at lower levels that aren’t captured by standard PGT-A.
Guidelines for prioritizing mosaics for embryo transfer
Different organizations have prepared guidelines for mosaic embryo transfer, including the PGDIS (Preimplantation Genetic Diagnosis International Society), ESHRE, and ASRM. Over time, these guidelines have changed as more data has become available.
Some of the first guidance came from the PGDIS in 2019 (Cram et al. 2019) and included specific chromosomes as part of their prioritization for mosaic embryo transfer (after mosaic levels), with preference being given to mosaics without chromosomes known to be involved in causing syndromes. They referenced Grati et al. (2018) for the ranking:
- Score 0 (highest priority for transfer): Mosaic trisomies 1, 3, 10, 12 and 19
- Score 1: 4, 5, (47, XXY)
- Score 2: 2, 7, 11, 17, 22
- Score 3: 6, 9, 15
- Score 4-5 (lowest priority for transfer): 8, 20, (47, XXX), (47,XXY)
- Not recommended: 13, 14, 16, 18, 21, (45, X)
Note that all the chromosomes listed here are trisomies, or 3 copies, because trisomies can generally survive while monosomies almost always die (exception is Turner syndrome as (45, X)).
The PGDIS updated their guidance in 2021 (Leigh et al. 2021) and moved away from chromosome-specific ranking, instead focusing on broader factors:
- Low level mosaic embryos are prioritized before high level mosaic embryos. They state that the percentage of mosaicism seems to be a better predictor for success than the actual chromosome involved.
- After the mosaic embryo’s level, they prioritize the embryo’s grade. Higher graded embryos tend to do better than lower graded embryos.
- After the grade, they prioritize the type of abnormality (segmental vs whole chromosome).
They also noted that the risk of having a baby with a chromosomal issue after mosaic embryo transfer appears to be low, and recommend prenatal testing for all pregnancies (with amniocentesis being the most accurate option). Read more in my post: PGDIS releases 2021 guidelines for mosaic embryo transfers.
More recent guidance from ESHRE (2022) and ASRM (2023) generally aligns with the 2021 PGDIS update.
- Level of mosaicism matters most. Lower-level mosaics are generally prioritized over higher-level ones
- Embryo quality still matters. Mosaic results shouldn’t be used on their own when choosing an embryo
- Chromosome-specific ranking is not reliable. There isn’t enough consistent data to prioritize embryos based on which chromosome is involved.
- Mosaic embryos are typically considered after euploid embryos. They are a reasonable option, especially when no euploid embryos are available, but tend to have lower success rates.
- Genetic counseling is strongly recommended. Mainly because results are uncertain and not always straightforward to interpret.
- Prenatal testing should be discussed for all pregnancies. Screening tests like NIPT have limitations for mosaicism, so diagnostic testing (like amniocentesis) is often recommended.
Can mosaic embryos lead to healthy babies?
Yes. Most mosaic embryo transfers result in healthy babies, and several studies have directly tested this.
- Viotti et al. (2023) compared miscarriage and neonatal outcomes for over 2,000 mosaic embryo transfers. They found birth outcomes (weight and gestational age) were similar to euploids, with no chromosomal abnormalities found in babies tested after birth. Read more in my post: Miscarriage and neonatal outcomes for over 2,000 mosaic embryo transfers.
- Morales et al. (2024) followed children born after mosaic transfers and found no differences in obstetric outcomes, with no health problems reported up to ~3 years of age. Read more in my post: Mosaic embryos show normal obstetric outcomes, healthy children up to 3 years old.
- Gill et al. (2025) examined outcomes when mosaic results were hidden during embryo selection and found no differences in obstetric or neonatal outcomes compared to euploid transfers. Read more in my post: Large study questions the value of reporting mosaic PGT-A results.
- Jin et al. (2026) showed that pregnancy complications and birth defects were not increased after mosaic embryo transfer, with some mosaic types (like segmentals) having outcomes similar to euploids. Read more in my post: Not all mosaics are equal: Researchers compare pregnancy outcomes by mosaic type.
Overall, these studies show that mosaic embryo transfers usually result in healthy babies, with similar birth and early childhood outcomes to euploid embryos.
Can mosaic embryos lead to mosaic babies?
Yes, it’s possible for mosaic embryos to result in a mosaic baby with the same abnormality — although it appears to be very rare.
As of 2023, there’s only been 7 case reports of this happening (to my knowledge). Larger studies give a better sense of how often this might happen. For example, a study of over 2,000 mosaic embryo transfers found that about 1.2% of pregnancies had prenatal test results matching the original mosaic finding (Viotti et al. 2023).
At the same time, most data is reassuring. Several studies that directly tested babies born after mosaic transfers found no evidence of the original chromosomal abnormality, even when using high-resolution methods or testing many cells.
Mosaic embryo transfers usually result in healthy babies, and confirmed cases of mosaicism in the fetus or baby appear to be rare. However, this may be underestimated, since abnormal cells can be present at very low levels or restricted to specific tissues that aren’t tested.
You can read more about this in my post: Can a mosaic embryo result in a normal baby?
How can a mosaic self-correct to become normal?
How is it possible for a mosaic embryo to lead to a normal birth without any signs of mosaicism? One potential mechanism is through a process called self-correction.
Self-correction is where a mosaic embryo is able to correct itself to become euploid. There are two possibilities for this (Spinella et al. 2018):
- The abnormal cells may die or grow more slowly, while the euploid cells survive or grow more quickly to eventually dilute the abnormal cells out.
- The abnormal cells might be displaced to the trophectoderm of the embryo (becomes the placenta), while the euploid cells are enriched in the inner cell mass (ICM).
Read more in my post: Depletion of aneuploid cells in mosaic embryos.
Are mosaics really mosaic?
This might sound like an odd question, but it’s important.
If a mosaic embryo is tested again, does it still come back as mosaic? Based on current evidence, not always.
PGT-A only samples about 5–10 cells from a blastocyst that may have hundreds of cells, so it’s not clear if this small sample represents the whole embryo.
Marin et al. (2021) showed that when embryos are rebiopsied:
- Euploid embryos usually test euploid again (~94%)
- Aneuploid embryos usually test aneuploid again (~81%)
- Mosaic embryos often give different results, with more than half not matching the original biopsy
Capalbo et al. (2021) also showed that:
- High-level mosaics more often test aneuploid
- Low and moderate mosaics usually test euploid on repeat biopsy
This shows that mosaic embryos don’t appear to be evenly mixed. Instead, they likely contain patches of abnormal cells within otherwise normal or abnormal tissue.
So depending on where the biopsy of a mosaic embryo is taken, you could get a mosaic result, euploid result or aneuploid result.
Read more in my post: Does a PGT-A biopsy match the rest of the embryo? A 2022 update
A study by Popa et al. (2025) also found that about a third of embryos labeled as mosaic by NGS were actually fully aneuploid when tested with a different method, suggesting some mosaic results may be misclassified. Read more in my post: A third of mosaics retest as aneuploid with different PGT-A test.
Mosaicism may change over time
Adding to all this, there’s evidence that a single PGT-A result might only represent the embryo at a single time.
Abdelbaki et al. (2025) used real-time imaging to watch embryos divide and found that chromosomal errors can continue to arise at the blastocyst stage, showing that mosaicism is a dynamic process.
This means that PGT-A results represent a snapshot in time, and an embryo’s chromosomal makeup may change as it continues to develop.
Read more in my post: Real-time imaging suggests that embryo mosaicism may change over time.
Success rates for mosaic embryos
Overall, mosaic embryos tend to have lower success rates than euploids, but still meaningful chances of pregnancy and live birth. Outcomes depend heavily on the level and type of mosaicism.
In general:
- Whole chromosome and complex mosaics tend to perform worse
- Low-level mosaics perform closer to euploids
- High-level mosaics have lower pregnancy and live birth rates
- Segmental mosaics often perform similarly to euploids
A really great study that looks at all this is by Viotti et. al (2021), where they evaluate outcomes from 1,000 mosaic embryo transfers. Overall they ranked mosaic embryos as follows:
- Segmental
- Low level (<50% mosaic), one chromosome affected
- Low level, two chromosomes affected
- Low level, complex (>3 chromosomes affected)
- High level (>50% mosaic), one chromosome affected
- High level, two chromosomes affected
- High level, complex

Read more in my post: Ranking 1,000 mosaic embryo transfers.
Capalbo et al. (2021) compared low (20-30% mosaic) and moderate (30-50%) mosaics:
- Euploid: 43.4% live birth rate
- Low level mosaics: 42.9% live birth rate
- Moderate level mosaics: 42% live birth rate
- Overall: no differences between euploids and low/moderate level mosaic embryo transfers.
- Read more in my post: No difference in euploid and mosaic embryo transfers: a clinical trial.
Viotti et al. (2023) analyzed over 2,000 mosaic embryo transfers:
- Mosaics (overall): higher miscarriage rates compared to euploids (22.2% vs 8.9%)
- Segmental mosaics: 41.7% ongoing pregnancy rate
- Whole chromosome mosaics: 28.2% ongoing pregnancy rate
- Read more in my post: Miscarriage and neonatal outcomes for over 2,000 mosaic embryo transfers.
Besser et al. (2024) found:
- Segmental aneuploids: 24.0% live birth rate
- High-level segmental mosaics: 43.1% live birth rate (no significant difference vs segmental aneuploids)
- Read more in my post: Segmental aneuploid embryos after PGT-A lead to healthy live births.
Jin et al. (2026) found:
- Mosaics (overall): lower live birth vs euploid (44.7% vs 51.7%) and higher miscarriage (18.1% vs 11.6%)
- Low level mosaics: similar outcomes vs euploid, increase in miscarriage
- High level mosaics: lower pregnancy and live birth rates vs euploid (61.8% vs 30.5%)
- Segmental mosaics: similar to euploids
- Whole chromosome (especially trisomy): worse outcomes compared to euploid
- Complex mosaics: lower success vs euploid
- Read more in my post: Not all mosaics are equal: Researchers compare pregnancy outcomes by mosaic type
Gill et al. (2025) showed that:
- Low level mosaics: 55.6% live birth (similar to euploids at 60.2%)
- High level mosaics: lower live birth (46.5%)
- Read more in my post: Large study questions the value of reporting mosaic PGT-A results
How useful are mosaic results?
Mosaic results can give extra information, but it’s not clear how helpful they are.
A large study by Gill et al. (2025) found that embryos could be selected just as well using standard factors like embryo quality, without knowing if the embryo was mosaic or not. They showed that mosaic status was a weaker predictor of success than embryo grading and didn’t improve the ability to predict live birth.
The authors noted that routine mosaic reporting may do more harm than good, as it can cause unnecessary stress or confusion for patients and may lead to viable embryos being discarded. They suggest that focusing on clearly aneuploid embryos might be a simpler approach for PGT-A.
Read more in my post: Not all mosaics are equal: Researchers compare pregnancy outcomes by mosaic type
Conclusions
Mosaic embryos are a mix of normal and abnormal cells and are a common result with PGT-A. Their chances of success can vary, but a pattern shows up across studies:
- Low level and segmental mosaics usually perform similarly to euploids
- High level, whole chromosome, and complex mosaics tend to have lower success rates
- Mosaic embryos can still lead to healthy babies, and confirmed mosaic cases in babies are rare
Because of this, mosaic embryos can be considered for transfer, especially when no euploids are available.
Armstrong et al. (2023) showed that including mosaics can also increase the number of embryos available for transfer, which may improve overall chances of pregnancy, especially for older patients.
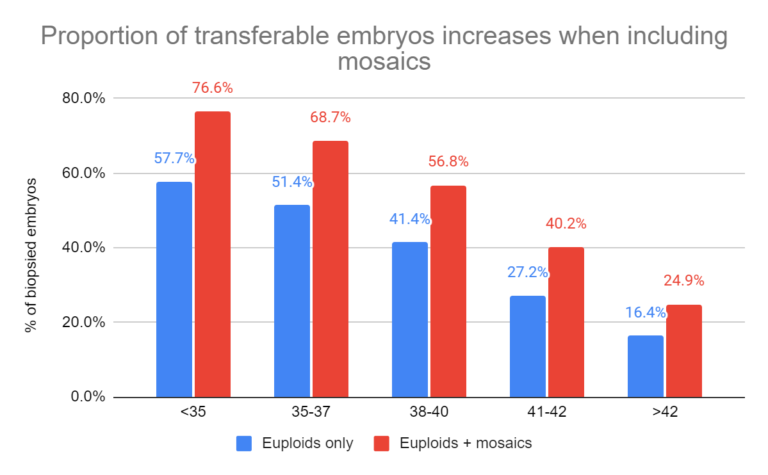
Read more in my post: A look at how PGT-A results change with age, using data from over 86,000 biopsies.
At the same time, mosaic results aren’t perfect. They’re based on a small biopsy and may not represent the whole embryo, with some research showing that mosaicism can change over time.
Overall, mosaic embryos fall somewhere in the middle: not as reliable as euploids, but still a good option, especially when there are no euploids available.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to PGT-A (PGS testing)
Complete guide to PGT-A (PGS testing)
 Ranking 1,000 mosaic embryo transfers
Ranking 1,000 mosaic embryo transfers
 No difference in euploid and mosaic embryo transfers: a clinical trial
No difference in euploid and mosaic embryo transfers: a clinical trial
 A look at how PGT-A results change with age, using data from over 86,000 biopsies
A look at how PGT-A results change with age, using data from over 86,000 biopsies
 How PGT-A testing has evolved (1990’s to today)
How PGT-A testing has evolved (1990’s to today)
 Large study questions the value of reporting mosaic PGT-A results
Large study questions the value of reporting mosaic PGT-A results
 Not all mosaics are equal: Researchers compare pregnancy outcomes by mosaic type
Not all mosaics are equal: Researchers compare pregnancy outcomes by mosaic type
 Depletion of aneuploid cells in mosaic embryos
Depletion of aneuploid cells in mosaic embryos