Mosaic embryos are able to self-correct and result in a normal baby the majority of the time, without evidence of any chromosomal abnormalities, however there are seven cases (as of 2023, to my knowledge) of a mosaic embryo leading to a birth with the same affected chromosome.
Mosaic embryos contain a mix of euploid (normal) and aneuploid (abnormal) cells. These abnormal cells can be reduced from the embryo by “self-correction” to result in a euploid embryo capable of producing a healthy baby. However, this isn’t always the case and there’s a risk of a mosaic embryo giving rise to a baby with the same chromosomal abnormality.
Check my complete guide to mosaic embryos to learn more about mosaics, or my complete guide to PGT-A to get more background on PGT-A (aka PGS testing).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
Mosaic embryos lead to chromosomally normal and healthy babies in most cases
Mosaic embryos can lead to chromosomally normal babies
Here’s a couple of studies I found that analyze the DNA of babies born after mosaic embryo transfers.
Capalbo et al. (2021) transferred mosaic embryos and tested the DNA of 38 newborns (11 from euploid transfers, 18 from 20-30% low level mosaic transfers and 9 from 30-50% moderate level transfers). All of the babies DNA was fully normal.
Gao et al. (2022) used single-cell multi-omics sequencing on seven infants born after a mosaic transfer. This is a high resolution technique that allowed them to sequence the DNA from individual cells. They sequenced the DNA from 1,616 blood cells from the 7 infants and didn’t find any of the original abnormalities in the newborns from the mosaic embryo transfers.
Viotti et al. (2023) reported on outcomes of over 2,000 mosaic transfers, with 8 babies that had a chromosome analysis after birth. All of them were normal.
Morales et al. (2024) found normal karyotypes of 6 children born after mosaic embryo transfer.
Mosaic embryo transfers lead to healthy babies
Viotti et al. (2021) transferred 1,000 mosaic embryos and studied their outcomes (summarized here). This study found a 37.0% ongoing pregnancy/live birth rate, representing about 370 ongoing pregnancies or live births. The authors noted that all newborns from these live births were healthy, and that a mosaic from any of the 23 chromosomes could result in a viable pregnancy.
Their complete list of mosaics that were transferred, along with their live birth outcomes can be found here (links to an excel spreadsheet from the study). Note that in this study they indicated <50% as a low level mosaic and >50% as a high level mosaic.
They noted that any of the chromosomes in mosaics were able to lead to a live birth without the affected chromosome, but they didn’t have enough data to do any analysis on individual chromosomes. So it’s not clear if one particular affected chromosome in a mosaic is more likely to miscarry, lead to a live birth, etc.
Viotti et al. (2023) reported on over 2,000 mosaic embryo transfers, resulting in 488 births with newborn data. Compared to euploids, the babies had comparable birth weights and length of gestation.
Morales et al. (2024) reported on 57 births from mosaic embryos and compared obstetric outcomes to euploids, finding no differences.
The PGDIS 2021 guidelines recommend always performing prenatal testing when transferring mosaic embryos.
Reports of mosaic embryo transfers leading to an affected fetus or baby
As of 2024, I was only able to find seven case reports where a mosaic embryo resulted in a baby with the same affected abnormal chromosome. Send me an email at embryoman@remembryo.com if you have any further information that I can add here.
Case report 1
Kahraman et al. (2020) detail a case report:
- PGT-A by next generation sequencing (NGS) diagnosed a mosaic monosomy 2 embryo with 35% mosaicism.
- Amniocentesis was performed at week 17 of pregnancy which revealed a mix of 46,XX cells (98% normal) and 47,XX,+2 cells (2% abnormal trisomy 2). Yes, trisomy and not monosomy 2 – see my note below.
- The fetus was monitored and there were no pathological findings at week 20 by ultrasound.
- Early rupture of the membranes led to a healthy female at 37 weeks. There were no signs of morphological abnormalities.
- DNA sequencing of the baby’s blood cells found 2% mosaic monosomy 2 (mos 45,XX,-2/46,XX) .
- DNA sequencing of buccal (cheek) cells found no mosaicism.
Note that here they saw trisomy 2 mosaicism after amniocentesis but monosomy 2 mosaicism in the embryo and baby. This is due to chromosomal non-disjunction, where one cell splits into two but doesn’t split the two duplicated copies of a chromosome equally during mitosis. In this case, one cell got one copy of chromosome 2 and the other cell got three copies (instead of two and two).
Mosaicism doesn’t have to be present in all the cells detected. Here they found mosaicism in the blood but not in the cheek. This may have to do with sampling error and not getting enough cheek cells, but it might also be due to how the cells divide and differentiate into different cell types.
All of the cells in our bodies have come from a single fertilized egg cell, which then divided into two cells, then four, etc. At some point these cells differentiated and went toward a specific lineage to become brain cells, intestinal cells, blood cells, cheek cells and more! It’s possible the cells in the embryo that had the monosomy 2 abnormality eventually went on to form blood cells, but not cheek cells.
Case report 2
The second case report (Greco et al. 2023):
- PGT-A by NGS diagnosed a segmental 40% mosaic embryo that contained a deletion spanning p36.33-p31.1 on chromosome 1.
- Amniocentesis was performed at week 17 which found a normal karyotype (46,XX).
- They then used a specific probe to detect abnormalities on chromosome 1 from the amniocentesis cells and found a deletion of the p36 region in 15% of cells.
- Genetic counselling was given and the possibility of severe intellectual development was discussed due to 1p36 deletion syndrome.
- The couple decided to terminate the pregnancy at 20 weeks.
- The products of conception were tested and the 1p36 segmental deletion was detected in 1.5% of brain cells (but not in the villi or heart).
Case report 3
The third case report (Greco et al. 2023):
- PGT-A by NGS diagnosed a complex mosaic (+1q(40%) -7(40%) -8(40%) +9(40%) -19(20%) -20(40%); +21(40%)).
- Chorionic villus sampling (CVS) at 8 weeks found mosaicism with chromosome 21.
- Noninvasive prenatal testing (NIPT) was performed at week 13 and chromosome 21 was found to be normal.
- Amniocentesis at around week 16 was performed and detected trisomy 21 in 16% of cells.
- Ultrasound at week 19 found a number of concerning pathologies which led to genetic counselling and the discussion of the possibility of trisomy 21 at birth.
- A level II ultrasound discovered a 8mm cystic formation and the couple decided to terminate the pregnancy at 22 weeks.
- A number of morphological features were discovered that were consistent with Dandy-Walker syndrome.
Case report 4
This case report is a bit different because it’s likely due to an inherited abnormality from one of the parents and wasn’t spontaneous. It also involved the transfer of a euploid embryo.
Mounts et al. (2019) detail the fourth case report:
- Two euploid embryos were transferred (PGT-A by NGS) which resulted in healthy twin boys being born.
- At 8 months of age, one of the boys was not meeting developmental milestones and was diagnosed with 15q duplication syndrome because of an extra copy of 15q11.2-q13.1.
- The original PGT-A results were confirmed euploid, but retesting the sample using a more sensitive PGT-A test (PGTai) found a high level 57% mosaic duplication on 15pter-q13.3.
- One out of three embryos retested with the same duplication, suggesting it was inherited.
Case report 5
This report is from a the Viotti et al. (2023) study, where over 2,000 mosaics were transferred. Of the 250 pregnancies with prenatal test results available, there were 3 cases (1.2%) where the prenatal test matched the PGT-A mosaic result:
- A low level complex mosaic with a trisomy 21 abnormality was confirmed and terminated.
- A low level segmental mosaic affecting chromosome 1 (1p36.33-p31.1) was confirmed and terminated.
- A low level segmental mosaic affecting two chromosomes (+4q32.2q34.3,-Xq27.3-q28) had the chromosome 4 abnormality confirmed by CVS. The pregnancy continued and resulted in a baby without birth defects.
You can check out the full review of this study in my post Miscarriage and neonatal outcomes for over 2,000 mosaic embryo transfers.
True mosaicism in babies is rare, but may be undetected
Levy et al. (2021) reviewed the incidence of mosaicism by a number of prenatal tests.
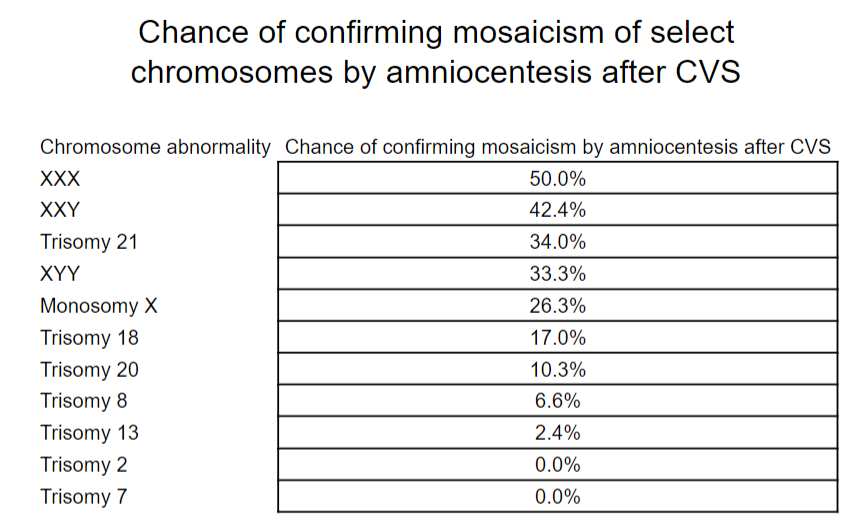
Mosaicism by CVS is about 1-2% in the general population and certain chromosomes are more likely to be confirmed by amniocentesis as shown below.
Huang et al. (2009) found similar rates of mosaicism by CVS among spontaneously conceived pregnancies and pregnancies involving infertility treatment (1.22% vs 1.32%).
Mosaicism by amniocentesis is about 0.2% and is rarely seen in the baby or products of conception (Levy et al. 2021). This may be because the mosaicism is completely gone, or there are a very low number of cells that aren’t detected, or because the mosaicism is restricted to a particular tissue that isn’t tested. This may result in “occult mosaicism” where mosaicism is suspected because there are clinical symptoms of a syndrome or disease, but it isn’t detected (Levy et al. 2021).
Mosaicism can sometimes be confined to the placenta, and this may be associated with pregnancy complications although this is controversial (Levy et al. 2021).
Conclusions
There are a large number of healthy births that have resulted from mosaic embryos. Mosaicism detected in the fetus or the baby appears to be very rare. Treff and Marin (2021) compiled 25 studies at the time which amounted to 2,759 mosaic embryo transfers, with only 1 confirmed mosaic in the resulting ongoing pregnancy (0.04%).
As of 2023, there are seven reported cases of mosaic embryos persisting to fetal mosaicism, but there could be more that just aren’t being reported or detected (or that I don’t know about!). This may be due to low numbers of abnormal cells, or mosaicism being restricted to a particular tissue that isn’t being tested. Limitations with PGT-A may also play a role, as only a few cells are sampled from a much larger embryo.
Regardless, mosaic embryos leading to mosaic babies with health problems does appear to be rare, as many healthy babies are born after these transfers, but the long term impacts of mosaic transfers are not yet known.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.