Researchers in a 2021 study found that women <35 who transferred 2 embryos against guidelines saw dramatic increases in multiple pregnancies, preterm births and low birth weights.
Women who transfer more than 1 embryo run the risk of having a multiple pregnancy. It’s risky because infants born from multiple pregnancies are more likely to have complications, as well as the mother during pregnancy.
The CDC reported in 2016 that 8.7% of singletons born from IVF were low birth weight compared to 54.9% of twins and 94.9% of triplets. Preterm births were also higher, with 13.7% among singletons, 64.2% among twins, and 97.0% among triplets.
Because of this, the ASRM and SART have issued guidelines to limit the number of embryos transferred. In some cases, transferring more than 1 embryo is acceptable, particularly at an older age. This is because the chances of a live birth are lower. The latest update to the guidelines can be seen here.
For women younger than 35, the recommendation is typically to transfer only a single embryo, except in special “non-favorable” circumstances. Despite this, in 2016, the CDC reported that women <35 transferred on average 1.5 embryos, with an elective single-embryo transfer (eSET) rate of only 42.7%.
A 2021 study by Gingold et al. compared obstetric outcomes from cycles where one embryo was transferred to cycles where 2 embryos were transferred (against guidelines). These women were <35 and had a “favorable” prognosis, meaning: first cycle of IVF, good embryo quality, and excess embryos available for cryopreservation. Blastocysts were transferred.
Since this is SART data, it was a pretty big data set! In all there were 15,643 fresh eSETs and 12,668 fresh non-eSETs. The majority of the multiple transfers were 2 embryos (99.5%), so from here on out I’ll be describing the non-eSET group as the double embryo transfer group.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Results
In terms of clinical pregnancies and live births, transferring 2 embryos did have higher rates:

But transferring two embryos dramatically increases the chances of having multiples. With a single embryo transfer, 96.5% of the births were singleton and 3.5% were twins, while with two embryos transferred 38.0% were singleton and 59.5% were twins:

Next, they looked at obstetric outcomes for those that transferred one embryo or more than one.
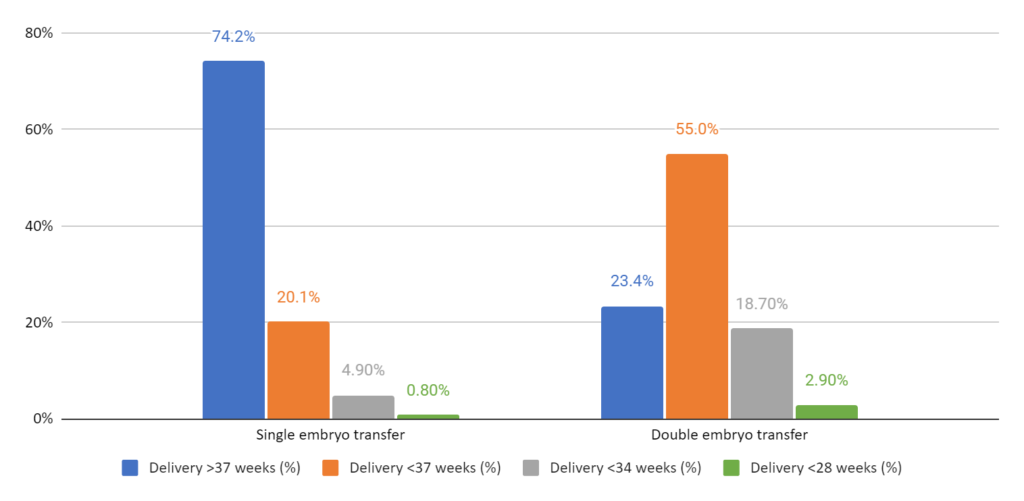
Deliveries occurred earlier and were mostly preterm when transferring more than one embryo (36 weeks vs 38 weeks). You can see the proportion of deliveries at <37 weeks, <34 weeks, and <28 weeks below. Note that babies born <28 weeks are extremely premature and are at a greater risk for complications and long-term health problems.
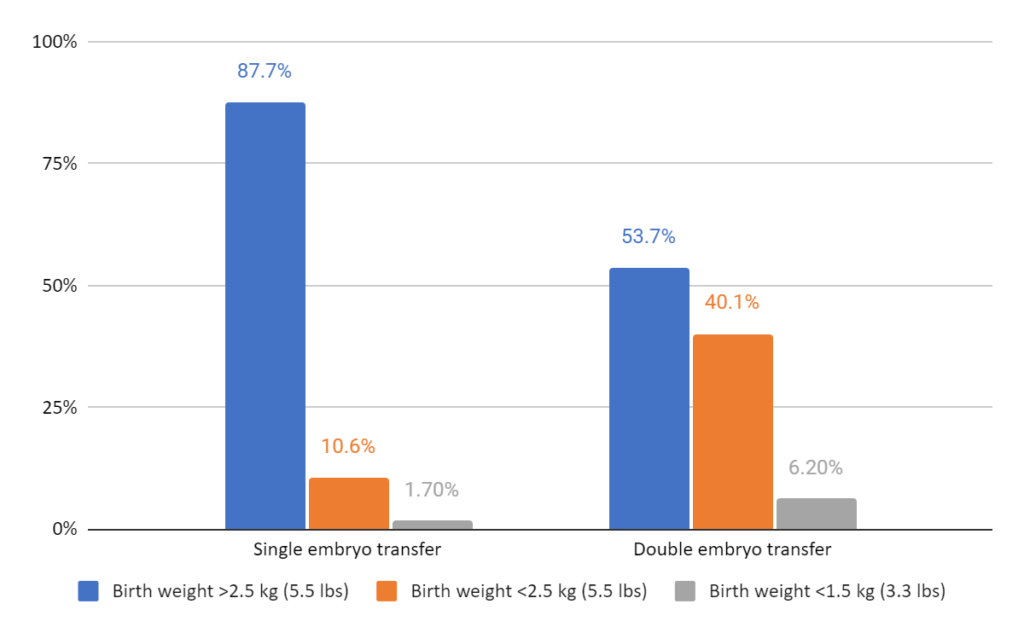
Birth weights were lower when more than one embryo was transferred. On average babies born from single embryo transfers were about 3.2 kg (7 lbs) compared to 2.6 kg (5.7 lbs) when more than one was transferred. There was a greater number of very low birth weight babies that were <1.5 kg (3.3 lbs) in those who transferred more than 1 embryo (6.2% vs 1.7%). These babies are at a greater risk for complications and long-term health problems.
The above data is for fresh transfers. This study also looked at frozen embryo transfers (2500 transfers) and found similar results:
- Higher live birth rate with double vs single embryo transfers (65.2% vs 58.9%)
- Greater proportion of multiples with double vs single embryo transfers (41.9% singleton/56.9% twins/1.2% triplets vs 95.2% singleton/4.8% twins/0% triplets)
- More preterm births with double vs single embryo transfers (about 35 weeks vs 38 weeks)
- Lower birth weight with double vs single embryo transfers (about 2.7 kg or 6 lbs vs 3.3 kg or 7.3 lbs)
And they looked at donor cycles! There were about 3500 of these cycles with similar results:
- Higher live birth rate with double vs single embryo transfers (69.1% vs 57.0%)
- Greater proportion of multiples with double vs single embryo transfers (31.3% singleton/67.6% twins/1.1% triplets vs 97.3% singleton/2.7% twins/0% triplets)
- More preterm births with double vs single embryo transfers (about 35 weeks vs 37 weeks)
- Lower birth weight with double vs single embryo transfers (about 2.8 kg or 6.2 lbs vs 3.2 kg or 7.1 lbs)
Conclusions
Transferring more than 1 embryo for women <35 with a favorable prognosis is not recommended based on ASRM guidelines (you can read about the latest guidelines here). Despite this many clinics will still transfer more than one embryo.
However, these are guidelines and there are good reasons for not performing a single embryo transfer. For some it might be a matter of cost. IVF can be extremely expensive, so transferring more than one embryo in a single procedure is usually a more cost-effective option.
There is sort of this myth about improving success rates by transferring more than one embryo. Everybody wants to transfer 2 embryos thinking that it will up their chances dramatically, and I don’t think that’s really true.
If you look back at the graphs, a single embryo transfer had a live birth rate of 52.7% and a double embryo transfer 61.6%. This is an 8.9% difference, which isn’t a whole lot. The better approach is to transfer one and get that 52.7% chance, and then if it doesn’t work try again with another 52.7% chance. This beats an improvement of only 8.9%, and it greatly reduces the risk of having multiples.
You might be wondering how the percentages add up! It’s not simply 52.7% and 52.7% because if it failed the first time there’s probably a lower chance of it working the second time.
In fact, there’s a study that looked at this! Crawford et al. (2016) looked at over 14k single vs double transfers in women <35. Women who had a single embryo transferred, AND had an extra embryo that they froze, had a 49.2% live birth rate. About 36% of women who had a failed transfer went on to have a live birth with their frozen embryo – representing a 68.8% cumulative live birth rate. Compare this to 57.7% live birth rate in women who transferred 2 embryos from the start. Transferring 2 embryos, one at a time sequentially, works better.
So much talk about the baby – what about the mother? Do multiple gestations have an impact on the mother?
Yes! Studies have shown that there’s a higher risk of preeclampsia, gestational diabetes, postpartum hemorrhage, and organ dysfunction (maternal near miss) in the mother (Santana et al. 2016). These issues may be exacerbated with maternal age (which is more likely an issue for those undergoing donor egg cycles).
So transferring one embryo works best – for mother and baby!
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 ESHRE 2023 guidelines on the number of embryos to transfer
ESHRE 2023 guidelines on the number of embryos to transfer
 How many embryos to transfer? 2021 ASRM recommendations
How many embryos to transfer? 2021 ASRM recommendations
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Researchers examine factors associated with preterm birth risk in IVF
Researchers examine factors associated with preterm birth risk in IVF
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols