Researchers in a 2023 study identified factors associated with preterm birth and found female BMI, AFC, multiple pregnancy, gestational hypertension and gestational diabetes to be independent risk factors. With this information, the researchers developed a tool to predict preterm birth risk.
Some studies have linked IVF to a higher rate of preterm births, but it’s not clear what factors influence this.
Wang et al. (2023) examined the association of different factors with preterm birth among women who performed IVF. They used this information to build a tool (a nomogram) that patients can use to predict their chance of a preterm birth. A total of 4,266 women were included in the study, 827 who had a preterm birth and 3,439 who didn’t, and involved cycles between 2016 and 2021 at a single IVF center in China.
Key information:
- This was a retrospective study.
- Sperm donation, PGT-M and PGT-A cycles were excluded.
- Preterm birth was defined as a live birth between 28 and 37 weeks gestation.
- A full-term birth was between 37 and 42 weeks.
The following variables were included in the analysis:
- Female age
- Male age
- Ethnicity
- Female and male education level
- Primary diagnosis for infertility
- Fresh or frozen transfer
- Female and male chromosome karyotypes
- Female and male body mass index (BMI)
- Antral follicle count (AFC)
- Anti-Müllerian hormone (AMH) levels
- ICSI or conventional IVF
- Thickness of endometrium
- Embryo transfer stage
- Number of embryos transferred
- Gestational hypertension
- Gestational diabetes
- Multiple pregnancy
- Smoking status
- Adverse pregnancy history (miscarriage, induced labor, ectopic pregnancy).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Variables associated with preterm birth rates
Of the 4,226 cycles included in this study, 827 had a preterm birth and 3,439 didn’t (the preterm birth rate was 19.39%).
A multivariate logistic regression analysis was done, which found statistically significant associations between preterm birth and:
- Female BMI
- AFC
- Multiple pregnancies
- Gestational hypertension
- Gestational diabetes
With multivariate logistic regression, these variables were found to be associated with preterm birth independently of the other variables. In other words, female BMI showed an association with preterm birth when all the other variables were controlled for and kept constant.
Let’s now look at each of these variables to get a sense of how much they impact preterm birth rates.
Preterm birth rate vs female BMI
Compared to women with a normal BMI (18.5-24.9), women that were overweight (25-29.9) and obese (>30) had an increased preterm rate (18.00% vs 23.81%, odds ratio [95% CI]: 1.366 [1.111-1.679]; 18.00% vs 26.29%, odds ratio [95% CI]: 1.537 [1.030-2.292]). Note: This means that for overweight women, the odds of having a preterm birth was 1.366 times higher than the odds for a woman with a normal BMI (or 36.6% higher).

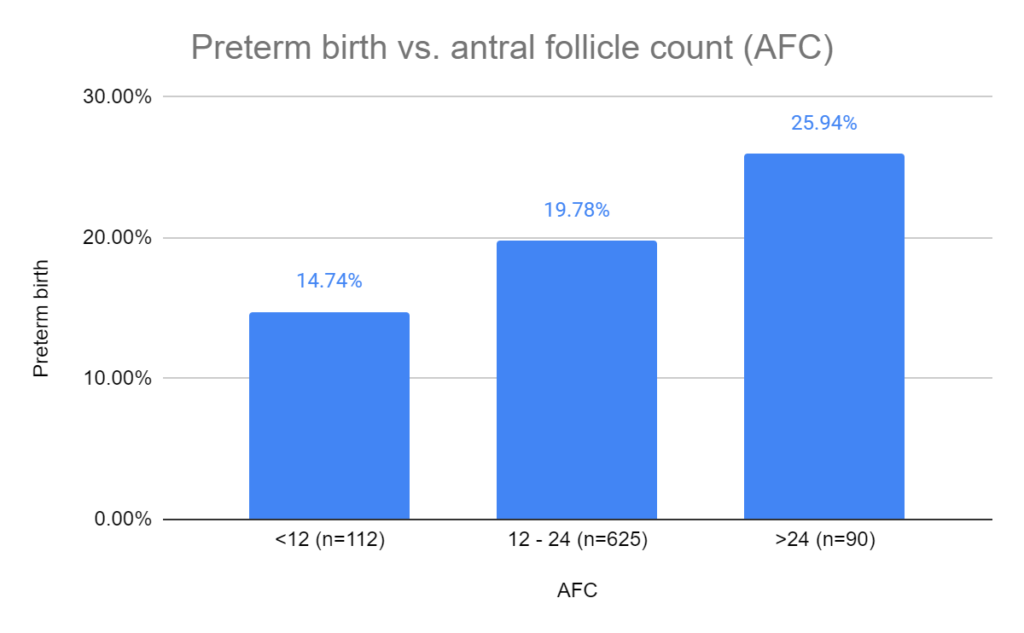
Preterm birth rate vs AFC
Compared to women with an AFC of 12 – 24, women with an AFC >24 had an increased preterm rate (14.74% vs 25.94%, odds ratio [95% CI]: 1.378 [1.030-2.292]).
Preterm birth rate vs multiple pregnancy, gestational hypertension and gestational diabetes
I grouped the last three together for simplicity.
Compared to women without a multiple pregnancy, women with a multiple pregnancy had an increased preterm rate (9.25% vs 42.10%, odds ratio [95% CI]: 6.744 [5.556-8.186]).
Compared to women without gestational hypertension, women with gestational hypertension had an increased preterm rate (17.48% vs 67.07%, odds ratio [95% CI]: 9.662 [6.632-14.078]).
Compared to women without gestational diabetes, women with gestational diabetes had an increased preterm rate (19.11% vs 46.51%, odds ratio [95% CI]: 4.650 [2.289-9.445]).

Nomogram to predict the chance of a preterm birth
Based on the five factors identified above, the researchers used this to construct a nomogram to help predict the risk of preterm birth. The ROC curve for this nomogram showed that is has a “relatively good prediction capability” with an AUC of 0.781.
The nomogram is below. To use it, you need to line up each variable and add up the points. So for a female BMI of 42, this would equal 60 points. The points are added up and the “total points” row can be used to draw a line to the preterm birth rate row. So if you had 200 points in total, then the risk of preterm birth would be about 0.8 or 80%.

Conclusions
This study found statistically significant associations with preterm birth and female BMI (overweight and obese), AFC (>24), multiple pregnancy, gestational hypertension and gestational diabetes. The most dramatic increase in preterm birth risk was seen in women with gestational hypertension (the odds were nearly 10 times higher).
The influence of BMI on preterm birth risk is well-established, and the authors suggest that a high antral follicle count (AFC), possibly associated with PCOS, may also contribute to the increased risk.
Both IVF and natural conception are prone to preterm birth with multiple pregnancies, highlighting the importance of mitigating this risk by opting for single embryo transfers in IVF.
While gestational hypertension is a common pregnancy complication, it occurs more frequently in IVF pregnancies compared to spontaneous pregnancies, and more research is needed to better understand this.
Although this study didn’t examine medicated vs natural FET, a recent meta-analysis found that medicated FETs have an increased risk of preterm birth vs natural FETs. You can read about that in my post Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes.
Limitations of this study include that it’s retrospective in design, was performed at a single center, didn’t explore the medical causes of preterm birth, and didn’t examine early preterm births.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 2 embryos or 1? The risks of a double embryo transfer for women under 35
2 embryos or 1? The risks of a double embryo transfer for women under 35
 ESHRE 2023 guidelines on the number of embryos to transfer
ESHRE 2023 guidelines on the number of embryos to transfer
 How many embryos to transfer? 2021 ASRM recommendations
How many embryos to transfer? 2021 ASRM recommendations
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols
 Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes
Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes