Researchers in a 2022 study created models to predict live birth rates and risk of multiples based on 223,377 embryo transfers in the US, and take into account the stage of embryo development (day 3 or day 5-7), the embryo’s quality/grade, whether the transfer is fresh/frozen and maternal age.
The authors used IVF clinic data from the US Society for Assisted Reproductive Technology (SART) between 2016-2018, consisting of 223,377 embryo transfers and 336,888 embryos. The authors used linear algebra to make best-fit models for live birth rates of embryos.
To learn more about day 3 (cleavage stage) and day 5 (blastocyst stage) embryo grading, check my Complete guide to embryo grading and success rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
How these models can be used
As we’ll see, this paper developed models for predicting live birth rates for single embryo transfers and transfers of more than 1 embryo (along with the chances of having multiples). This information is useful for a number of reasons:
- Patients can get realistic statistics for transferring embryos of a particular grade/quality based on their age and the number transferred.
- Doctors can counsel patients before starting IVF, or once they have frozen embryos to transfer.
- Doctors can determine the safe number of embryos to transfer to avoid multiples.
- Clinics can use this information in establishing performance metrics (by summing the predicted live birth rates of embryos), which can be useful in evaluating an IVF stimulation protocol, a frozen embryo transfer protocol, or embryo culture performance.
Limitations of these models
To be clear, this paper is not presenting the actual data that was reported by SART but models that best fit the data to a curve. These models are a prediction tool to help doctors and patients as indicated above. Because there were sometimes gaps in the data, or outliers, they used “moving averages” to smooth the data out. So for the age 30 with a 5-year moving average, they would have averaged the values for ages 28, 29, 30, 31 and 32 to give the value for age 30.
The majority of data they presented were from embryos with 8 cells (day 3), or blastocysts that were good quality (day 5-7). For day 3 embryos, 48% had 8 cells, 18% had >8 cells, 12% had 6 cells, 11% had 7 cells, 6% had 5 cells and 6% had 4 cells. For blastocysts, 76% were good quality, 21% were fair quality and 3% were poor quality. You can see the distributions below.
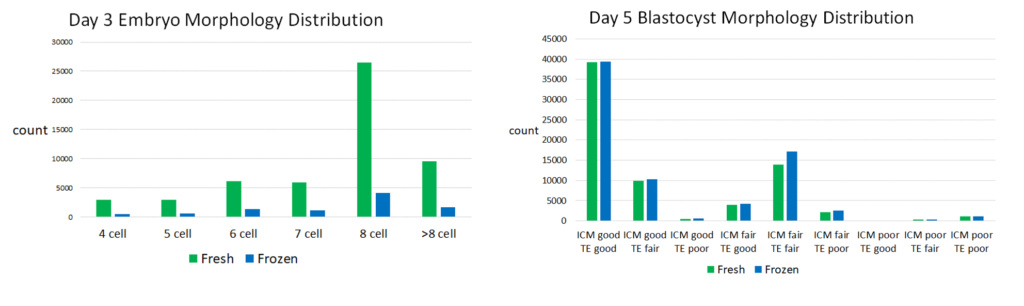
They also modeled live birth rates for fresh and frozen embryo transfers, and for the most part there were more frozen transfers compared to fresh. The lower sample size for some of this data might explain why the fresh and frozen models trend a bit differently, so keep this in mind.
Here’s the distribution of fresh/frozen transfers based on the 223,377 embryo transfers:
- Fresh day 3 cleavage 14.7%
- Frozen day 3 cleavage 3.1%
- Fresh day 5 blastocyst 28.5%
- Frozen day 5 blastocyst 35.8%
- Fresh day 6 blastocyst 0.9%
- Frozen day 6 blastocyst 16.3%
- Fresh day 7 blastocyst 0.04%
- Frozen day 7 blastocyst 0.6%
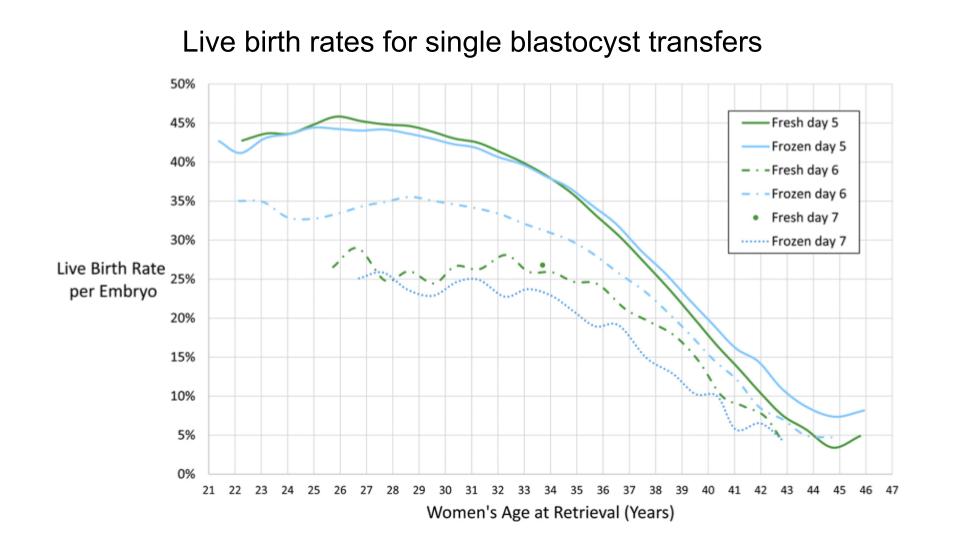
Blastocyst stage (day 5-7) single embryo transfers
The first model we’ll look at is for blastocyst transfers. We can see that for ages up to about 33-35 the live birth rates are consistent for each embryo stage (day 5-7). Notice that there seems to be an improvement in live birth rates with frozen transfers in women >40 compared to fresh transfers. The authors noted that this is a new finding and worth further examination in a randomized controlled trials (RCT).
Live birth rates by blastocyst grade/quality
In terms of quality, they compared expansion (early blast, expanding blast or hatching blast) and quality, which was expressed in terms of the overall embryo grade (good/fair/poor) or as individual quality grades for the ICM/trophectoderm (good/fair/poor).
If you’re unclear on what this means, check out my post on blastocyst grading.
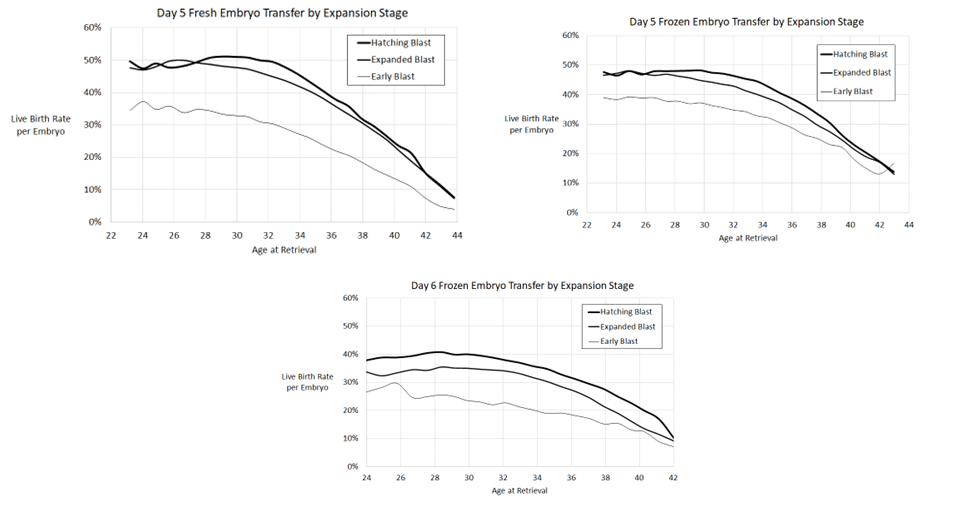
Blastocyst expansion
Here they included the day 5 fresh (top left) and frozen (top right) as well as day 6 frozen (bottom) models. Presumably day 6 fresh, and day 7 fresh and frozen, weren’t included because of the smaller sample size.
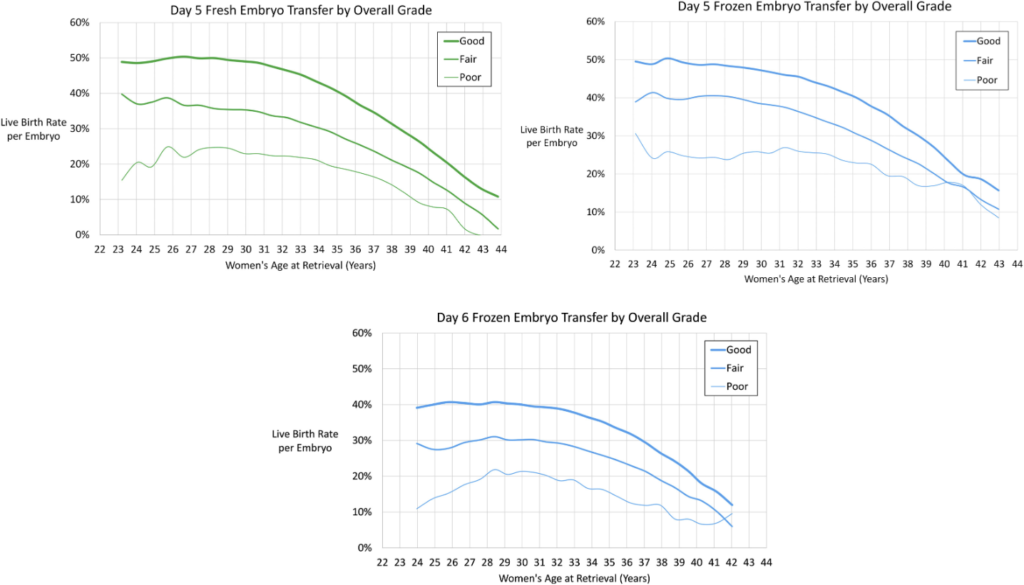
Blastocyst quality (overall grade)
When reporting data to SART, clinics can choose the quality of the embryo as good/fair/poor overall. How clinics determine this is up to the clinic, but but embryos with AA are good, BB are fair, and CC are poor. Embryos that are AB may be considered good or fair, and BC may be considered fair or poor (this is up to the clinic!).
Here they included the day 5 fresh (top left) and frozen (top right) as well as day 6 frozen (bottom) models. Presumably day 6 fresh, and day 7 fresh and frozen, weren’t included because of the smaller sample size.
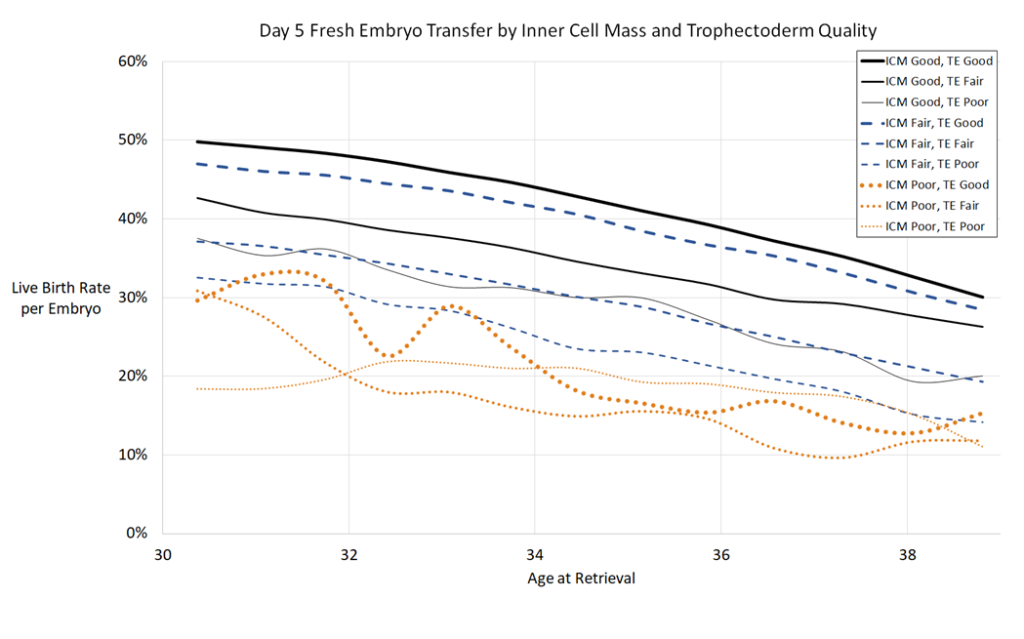
Blastocyst quality (ICM/trophectoderm grades)
Next they made models based on individual ICM and trophectoderm grades. Remember that A=good, B=fair and C=poor, and that a 4BA has a fair ICM and a good trophectoderm.
I think it’s worth pointing out that some clinics don’t grade early blasts because the ICM and trophectoderm aren’t fully developed. So in the case of an early blast, it may be best to use the models for expansion above. The following models are more for expanding/hatching blasts, which follow each other pretty closely in the expansion models.
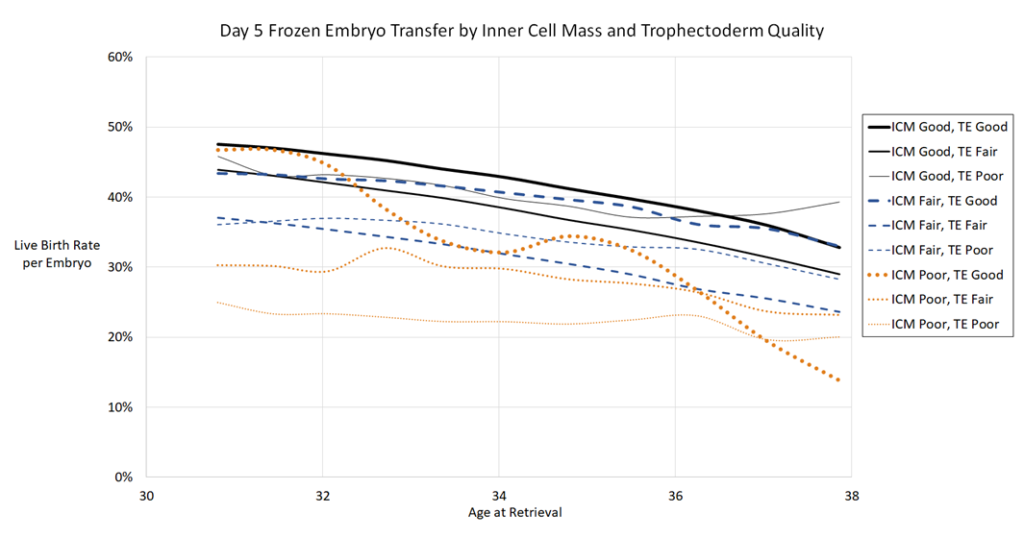
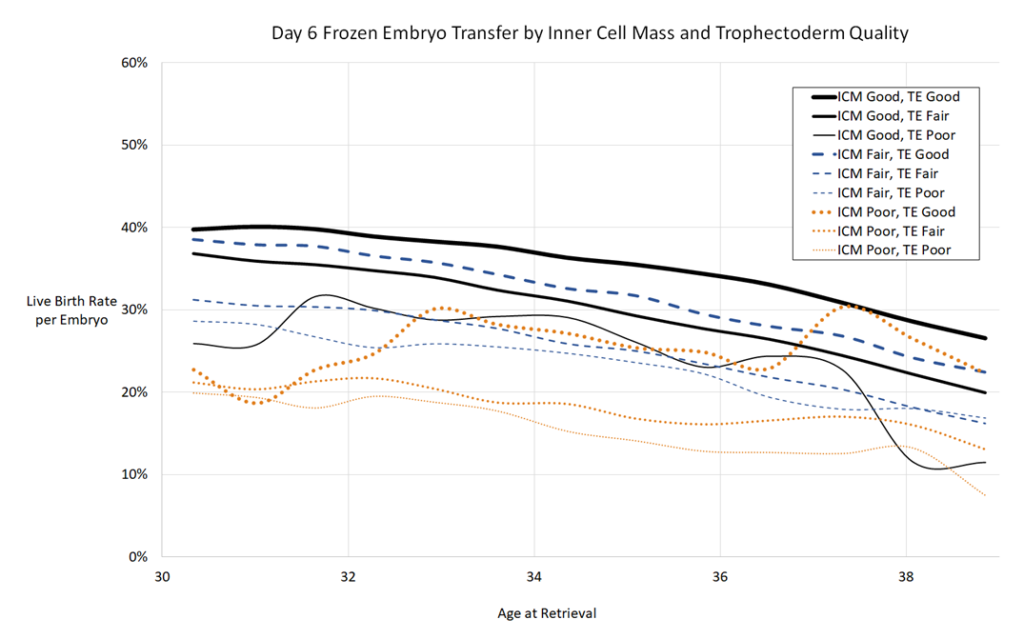
The first graph is day 5 fresh, then frozen, then day 6 frozen. You’ll notice that some of the lines jump around a bit, particularly for poor quality embryos. Remember that most of the data was based from good quality embryos, so any anomalies may be due to the smaller sample size as indicated above.
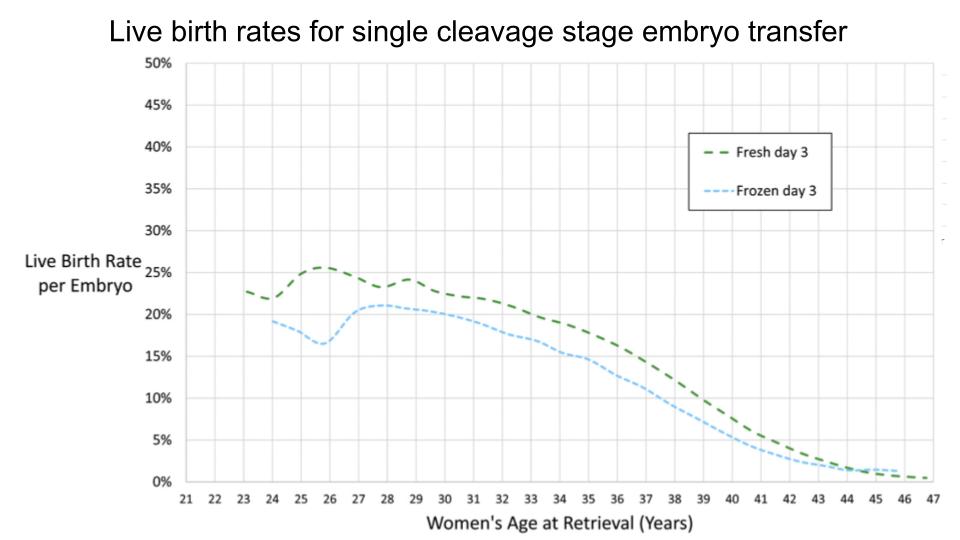
Cleavage stage (day 3) single embryo transfers
Next they looked at day 3 cleavage stage embryo transfers. On average, these were predicted to be about half as likely to produce a live birth compared to day 5 embryos. The authors noted that of the 356 single day 3 embryo transfers in women between 45-52, there were no live births.
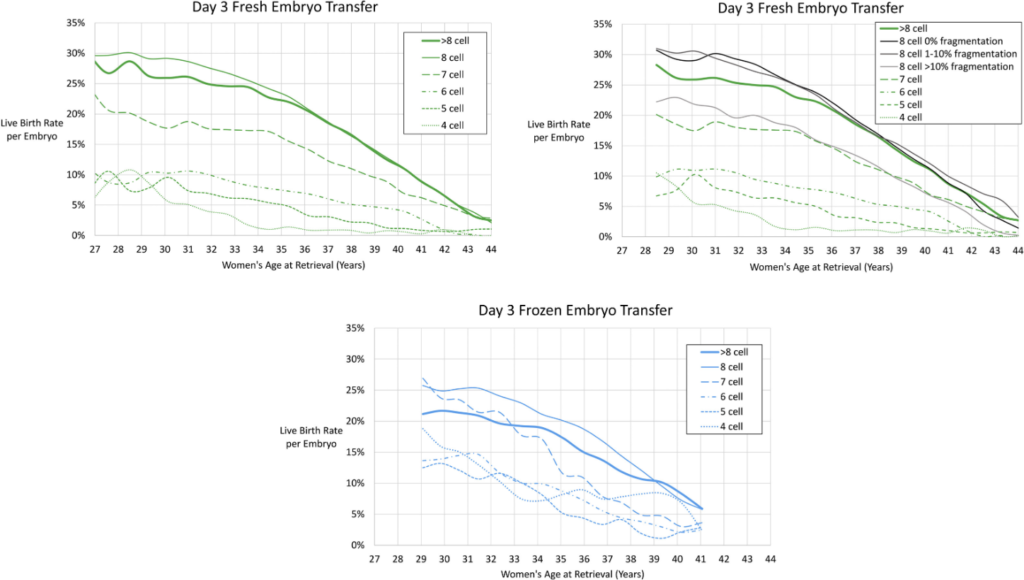
Live birth rates by cleavage stage embryo quality/cell number
While there is some consistency with how blastocysts are graded, day 3 embryos can be graded differently. One recurring theme, however, is cell number and fragmentation. Typically 8 cells is considered ideal, although there is evidence that >8 cells is similar and fragmentation <10% is usually best. Using the SART system, good quality embryos have <10% fragmentation, while fair and poor quality embryos have 10-25% and >25% fragmentation respectively.
For more information, check out my post on cleavage stage embryo grading.
Here they included models for day 3 fresh transfers based on cell number (top left) and fragmentation (top right) as well as models for day 3 frozen transfers based on cell numbers (bottom). Presumably the model for day 3 frozen transfers based on fragmentation weren’t included because of a smaller sample size.
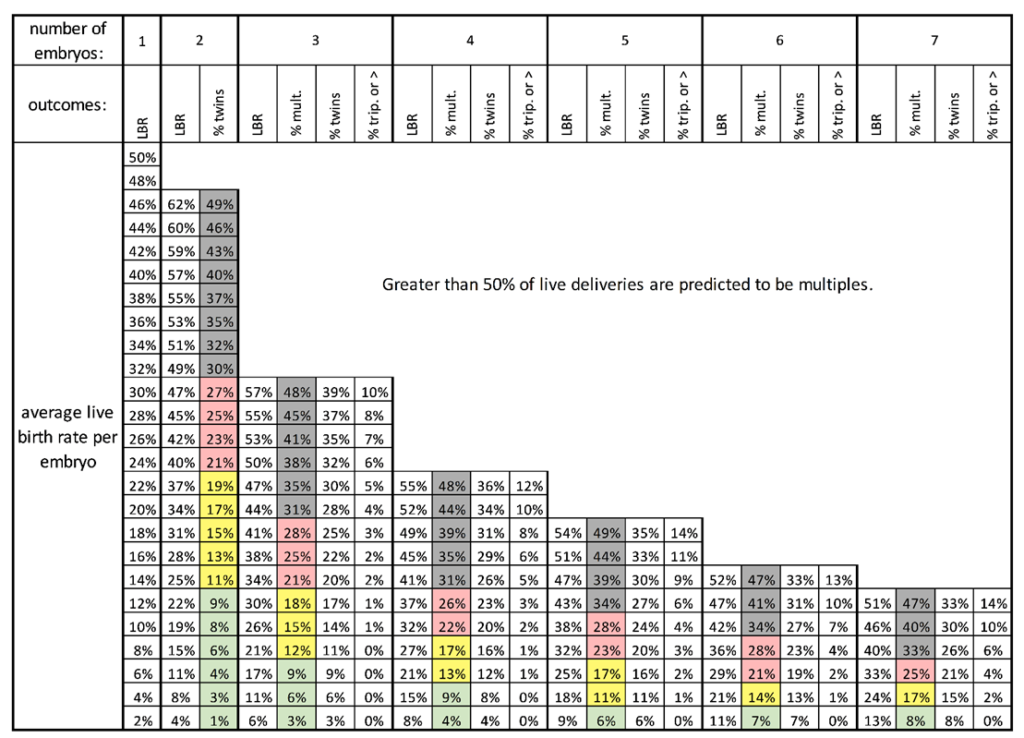
Transferring 2 or more embryos and predicting live birth rates and risk of multiples
In addition to providing models that can be used to predict live births for single embryo transfers as shown above, the authors also included a chart for determining live birth rates after transferring more than one embryo and the risk of multiples.
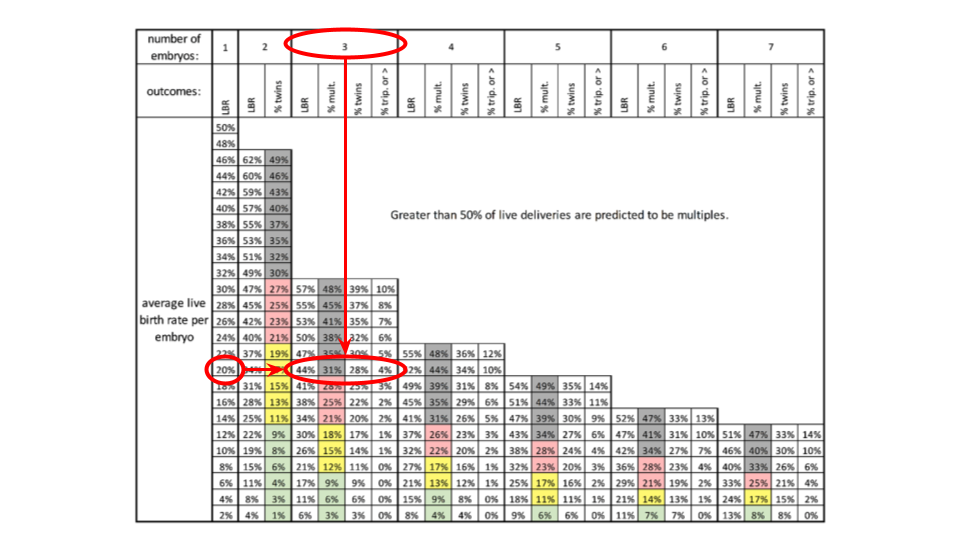
To use this chart, let’s look at an example of 3 embryos being transferred. You can determine the chance of live birth for each embryo (based on age, grade, etc.) by following the models above. Let’s say we’re looking at a 38 year old who wants to transfer 3 day 5 fresh blastocysts: a 4AA (live birth rate ~ 33%), a 3BC (LBR ~ 15%), and a 3CB (LBR ~ 11%).
- Average = (33% + 15% + 11%) / 3 = 20%
- From the left of the chart, find 20%
- From the top of the chart, find 3 (because 3 embryos are being transferred)
- The corresponding box gives a live birth rate of 41%, a chance of multiples of 28%, a chance of twins at 25%, and a chance of triplets or higher at 3% (see below)
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Predicting how many day 3 embryos make it to blastocyst
Predicting how many day 3 embryos make it to blastocyst
 Transferring a good and poor quality embryo together: a meta-analysis
Transferring a good and poor quality embryo together: a meta-analysis
 AI model predicts live births from blastocyst images with highest accuracy yet
AI model predicts live births from blastocyst images with highest accuracy yet
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?