Researchers in a 2022 study found no benefit in patients who used the ERA after transferring a single euploid, even when accounting for a history of failed transfers.
The endometrial receptivity array (ERA, see here for more information) is a technique that is believed to improve implantation rates by determining the optimal time for transfer (the window of implantation), based on a molecular analysis of a uterine biopsy. Whether or not it works is not clear, as most studies are small, use tested and untested embryos, and a mix of other variables.
Doyle et al. (2022), in the largest ERA study to date, performed single euploid frozen embryo transfer (FET) cycles based on either standard practice (123 ± 3 hours progesterone, 2284 FETs) or timing determined by the ERA (307 FETs). This study was retrospective and used data from 2018 and 2019. ERA results were “receptive” if they fell between 123 ± 3 hours progesterone, and “nonreceptive” if a different timing was determined. In this study, 59.3% of patients were nonreceptive (182 patients).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
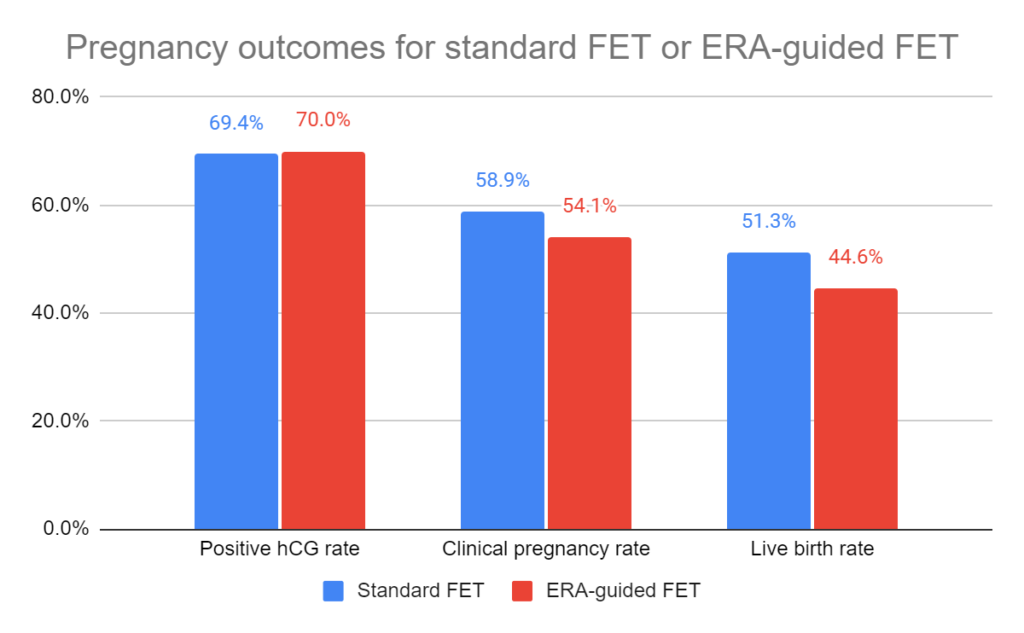
The ERA didn’t improve outcomes compared to standard FET
After transferring a single euploid in ERA-timed patients (307) vs standard FET patients (2284), there was no statistically significant change in positive hCG (70.0% vs 69.4%), clinical pregnancy (54.1% vs 58.9%) or live birth rates (44.6% vs 51.3%).
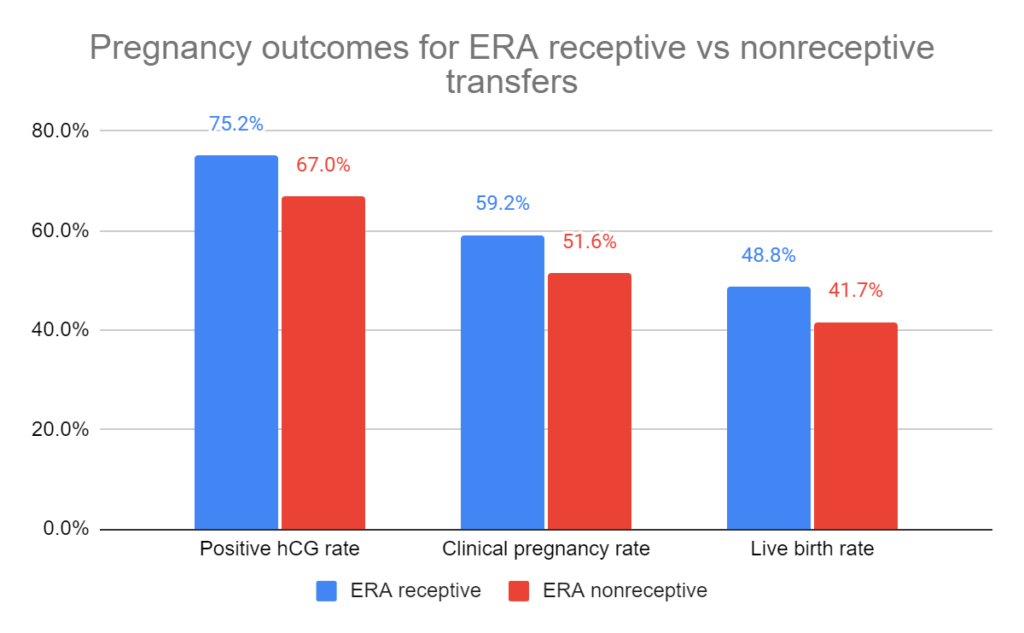
The ERA didn’t improve outcomes between ERA receptive and non-receptive patients
After transferring a single euploid in ERA receptive patients (125) vs ERA nonreceptive patients (182), there was no statistically significant change in positive hCG (75.2% vs 67.0%), clinical pregnancy (59.2% vs 51.6%) or live birth rates (48.8% vs 41.7%).
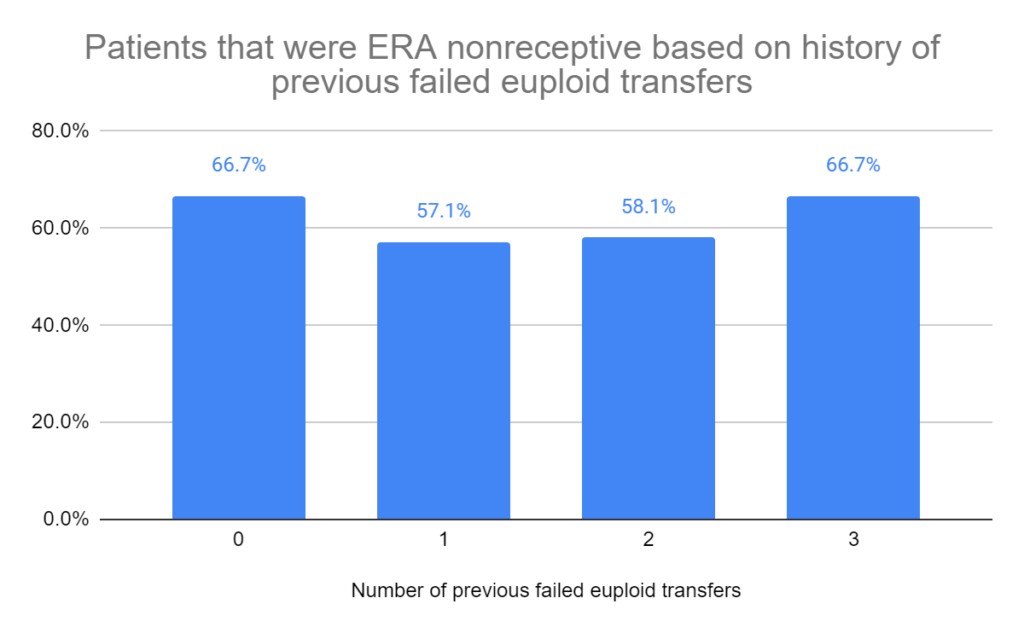
Women with a history of failed transfers showed equivalent receptivity by ERA
Next, they grouped the ERA patients based on their history of failed euploid transfers for both receptive (total = 125; 0 failed transfers = 16; 1 = 70; 2 = 34; 3 = 5) and nonreceptive patients (total = 182; 0 failed transfers = 32; 1 = 93; 2 = 47; 3 = 10). They found that women with an increased number of failed transfers weren’t more likely to have a nonreceptive ERA result.
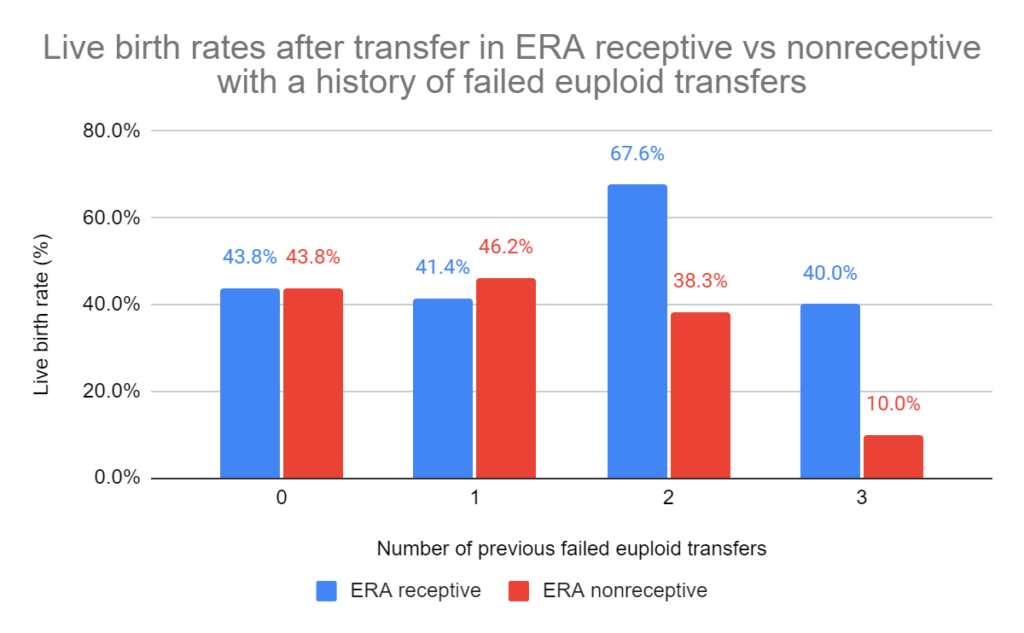
Adjustment by ERA didn’t improve outcomes with history of failed transfers
Generally, there were no improvements when considering the number of previous failed euploid transfers. There was a statistically significant increase in live births in receptive patients (who didn’t require an adjustment of progesterone timing) with a history of 2 failed euploid transfers, compared to nonreceptive patients. According to the authors, the sample size was too low to draw a clinically meaningful conclusion. The group with 3 failed transfers wasn’t statistically significant (but had a low sample size as shown above).
Conclusions
This study didn’t find any differences between positive hCG, clinical pregnancy and live birth rates after euploid transfers guided by the ERA or by standard protocols. They also found no differences between ERA receptive and nonreceptive patients.
The authors mention that there may not be differences with the ERA because adjusting progesterone in nonreceptive ERA patients may boost their success rates to that of the receptive patients. However, if this is truly the case then patients who used a standard FET (which would include a similar proportion of nonreceptive patients) should have lower outcomes compared to the ERA group.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Meta-analysis finds no difference in pregnancy outcomes when using the ERA
Meta-analysis finds no difference in pregnancy outcomes when using the ERA
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer
 IVF pregnancy outcomes after intrauterine PRP: a 2022 clinical trial
IVF pregnancy outcomes after intrauterine PRP: a 2022 clinical trial
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
 Intrauterine hCG for IVF patients improves pregnancy rates
Intrauterine hCG for IVF patients improves pregnancy rates
 Meta-analysis finds mixed results for ERA and other receptivity tests
Meta-analysis finds mixed results for ERA and other receptivity tests