Researchers in a 2024 study found that patients with higher systemic inflammation had reduced live birth rates and increased pregnancy loss rates, potentially identifying a group of patients that might benefit from immunotherapies during IVF.
The systemic immune-inflammation index (SII) is a biomarker for inflammation and is based on neutrophil, lymphocyte and platelet counts from a blood sample. Higher SII levels indicate a higher degree of inflammation in the body. Studies have shown that SII is related to disease severity for cancer, COVID-19 and heart disease (Ma and Li 2023), but it isn’t clear how SII relates to IVF outcomes.
In this study, researchers grouped patients from low to high SII levels, and report their live birth rates and pregnancy loss rates after their first IVF. They wanted to see if patients with high systemic inflammation have decreased live birth rates and increased pregnancy loss rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This is a reotrospective cohort study that took place between 2018 and 2020 at a single hospital-based IVF clinic in China.
- This study included the patient’s first IVF cycle. They all had a GnRH-antagonist cycle, were aged 20-40 years old and had a fresh transfer.
- SII was measured using a blood sample from the day before egg retrieval. SII was defined as the platelet count x (neutrophil count / lymphocyte count).
- Exclusions: PCOS, hyperprolactinaemia, thyroid dysfunction or other endocrine-related disorders, history of ovarian surgery or endometriosis diagnosed by transvaginal sonography, complications with liver, kidney or thyroid dysfunction, recurrent spontaneous miscarriage, congenital or acquired uterine malformations, abnormal parental karyotypes.
- Only the first fresh transfer was considered, with up to two day 3 or 5 embryos transferred (most transfers involved transferring 2 day 3 embryos).
- The primary outcome was the live birth rate and early pregnancy loss rate (which included miscarriage/ectopic pregnancy before 12 weeks).
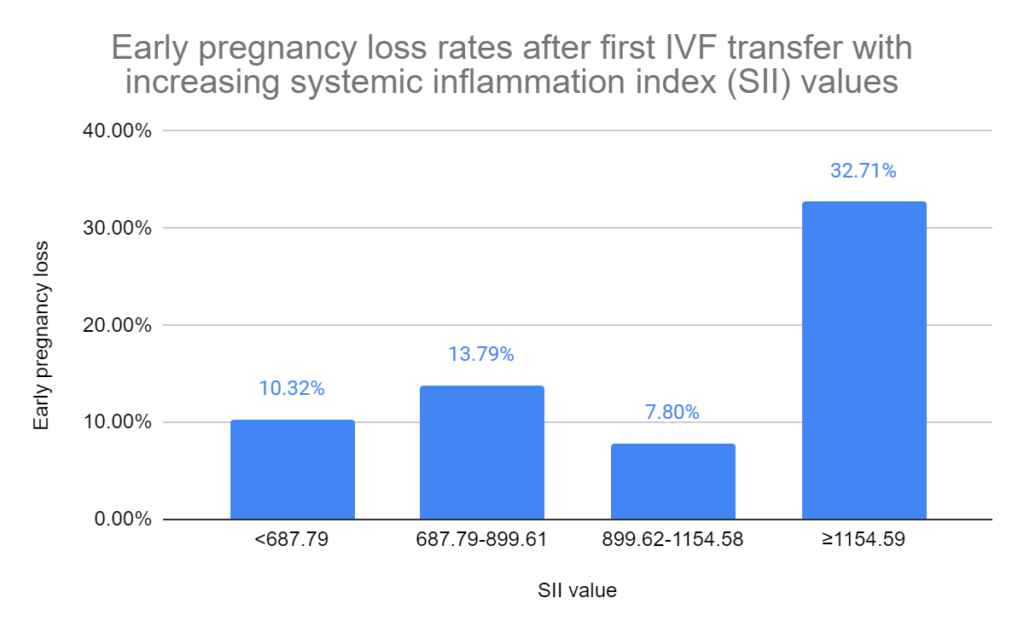
In terms of sample size, there were a total of 1,188 patients in this study. The patients were divided into four groups (quartiles) based on their baseline SII values: <687.79; 687.79-899.61; 899.62-1154.58, ≥1154.59.
In terms of baseline characteristics, there were differences between the groups’ age (range was 31.97 to 32.95), starting gonadotropin dose, total gonadotropin dose (range was 2100 IU to 2225 IU) and hCG value at 12 h after trigger. These were statistically adjusted in their statistical model, along with infertility duration, number of spontaneous miscarriages, BMI, duration of GnRH antagonist, total GnRH antagonist dose, endometrial thickness on trigger day, and estradiol/progesterone on hCG start day.
There were no differences in baseline characteristics for IVF outcomes between the SII groups: number of eggs retrieved, number of fertilized eggs, number of cleavage embryos, number of embryos transferred, number of superior quality embryos, number of blastocysts, blastocyst formation rate, stage of embryos transferred, ICSI vs IVF, etc.
With increasing SII, live birth rates decrease while early pregnancy losses increase
This study split up the patients into four groups (quartiles) with increasing SII and compared pregnancy outcomes between the groups.
Patients with the highest SII values had lower live birth rates compared to patients with the lowest SII values (24.24% vs 46.80% p< 0.001; adjusted odds ratio [95% CI]: 0.39 [0.27-0.56]). This means that after statistical adjustment, patients with the highest SII had 0.39 times the odds live birth rate of those with the lowest SII. After adjustment, there were only differences between the lowest and highest SII groups.

They also looked at early pregnancy loss rates (miscarriages/ectopic pregnancies before 12 weeks). Patients with the highest SII had increased early pregnancy loss rates compared to those with the lowest SII (32.71% vs 10.32%, p< 0.001; adjusted odds ratio [95% CI]: 2.27 [1.21-4.28]). This means that after statistical adjustment, patients with the highest SII had 2.27 times the odds of early pregnancy loss rate of those with the lowest SII. After adjustment, there were only differences between the lowest and highest SII groups.
SII values can range quite a bit between individuals, making the distribution of data skewed. To address this, the researchers used the log of the SII values to make the distribution more symmetric and to help model the data. By modeling the data in this way, they identified a cut-off for SII values where rates started decreasing. This was at 6.72 for the biochemical pregnancy rate. The antilog of 6.72 is over 5 million, so I’m assuming they’re using the natural log here (with a base of e), which puts the SII cutoff at about 829. This is the SII value where biochemical pregnancy rates start to decrease. They found similar results with other pregnancy outcomes around this same cut-off.
Conclusions
This study found that patients with the highest SII level (≥1154.59) had lower live birth rates compared to those with the lowest SII level (<687.79).
The highest SII group also had an increased chance of early pregnancy loss before 12 weeks. The cut-off for decreased pregnancy outcomes was 829.
This is the first study to look at SII values and relate it to IVF pregnancy outcomes.
SII is a marker for inflammation, and has been linked to disease severity. High SII could potentially affect egg quality and endometrial receptivity. Studies have shown that SII is associated with miscarriage and preterm pre-labour rupture of membranes.
The researchers say that this might be a good way to identify patients that would benefit from immune therapies. Measuring SII is relatively easy and only involves a blood sample the day before the retrieval.
However, without actually testing if patients with high SII benefit more from immunotherapies compared to low SII patients, it’s just speculation. Hopefully in the future they actually test this out to see!
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (3 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 RCT finds no benefit for prednisone use among RIF patients
RCT finds no benefit for prednisone use among RIF patients
 Contamination linked to repeated failed transfers, patient has live birth after zona removal
Contamination linked to repeated failed transfers, patient has live birth after zona removal
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 β-hCG levels and biochemical pregnancy loss
β-hCG levels and biochemical pregnancy loss
 Can sperm and egg be “genetically incompatible”?
Can sperm and egg be “genetically incompatible”?
 POPI-Plus calculator predicts chance of live birth after positive beta-hCG
POPI-Plus calculator predicts chance of live birth after positive beta-hCG