Researchers in a 2024 study found that recurrent implantation failure patients with underlying immunological issues had improved live birth rates after receiving immunotherapies, such as prednisolone, heparin and/or intralipids.
This study wanted to see the impact of different immunotherapies on patients with recurrent implantation failure (RIF) and underlying immunological issues (aka immunological RIF). They tested up to three different immunotherapies, including corticosteroids (prednisolone), low molecular weight heparin (LMWH) and/or intravenous intralipids.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a multicenter, retrospective study that involved 15 fertility clinics in the UK between 1997 and 2018.
- The patients had RIF (with at least two failed embryo transfers) and evidence of an immunological issue.
- Immunological issues included: a high titer of autoimmune antibodies, high numbers/ratios of T of B cells, or high numbers/activity of peripheral NK cells.
- The control group included patients who declined immunological testing or tested negative for any immunological problems.
- Patients were treated with corticosteroids (prednisolone), LMWH and/or intravenous intralipids, as a single treatment or combination dual/triple.
- Donor egg cycles were permitted.
- Cleavage stage or blastocyst stage embryos were transferred (average was about 2 in both groups).
- The primary outcome was live birth rate.
In terms of the sample size, there were 5,083 cycles that received immune treatment and 22,080 that didn’t.
In terms of the patient characteristics, the patients who received immune therapy vs the control group were older (38.5 vs 37.1), more likely to have a frozen embryo transfer (29% vs 17.6%) or egg donation (11.7% vs 8.5%), along with other differences. These confounders, along with the different immunotherapies used, were statistically adjusted in their statistical models (toward the end of the article– the majority of the stats in this article weren’t adjusted).
Immune protocols used
Different immunotherapies were prescribed, either a single, dual or triple therapy, depending on 1) autoimmunity, 2) dysfunctional T or B cells, 3) abnormal NK cell cytotoxicity or 4) abnormal Th1/Th2 cytokine profiles. In most cases, a dual or triple therapy was used, but if there were risks of side effects for a particular immunotherapy (or based on patient preference), than only a single therapy was used.
Let’s take a closer look at the different tests they did to establish evidence of an underlying immunological abnormality, along with the corresponding immune protocol used.
1) Autoimmunity
- This test included autoimmunity measured by high titers (levels) of Anti-thyroid peroxidase (Anti-TPO) antibodies, Antinuclear antibodies (ANA), Anti-smooth muscle, Antibodies (ASMA), Anti-mitochondrial antibodies (AMA), Anti-phospholipid antibodies (APL) and Anti-gastric parietal cells antibodies.
- A dual therapy was offered including 1) 40 IU/day of LMWH from 2 days before transfer to 12 weeks gestation and 2) 10 mg/day of prednisolone from the start of treatment to 20 mg/day from the embryo transfer day until 12 weeks gestation.
2) Abnormal lymphocytes (B, T and NK cells – based on their numbers and ratios):
- Lymphocytes were measured using different markers: CD19 (B cells), CD3 (T cells) and CD56 (peripheral NK cells).
- Patients with abnormal B/T cells were offered the LMWH/prednisolone dual therapy as above. Patients with a slight NK cell increases were offered LMWH/prednisolone and optional intralipids and IVIG. Note that the study didn’t mention any further details about IVIG, so I’m assuming not many patients used this treatment.
3) Abnormal NK cell cytotoxic activity
- NK cell cytotoxicity (killing ability) was measured by incubating patient NK cells with trophoblast-like cells with or without immunotherapies (prednisolone/IVIG/intralipids).
- Patients with higher NK cell increases or cytotoxic activity were offered the triple therapy LMWH/prednisolone/20% intralipids (100 ml) on day 4-9 of the cycle.
4) Abnormal Th1/Th2 cytokine ratio
- Th1/Th2 cytokine levels were measured using TNF-alpha or IFN-gamma (Th1 cytokines) and IL-10 (Th2 cytokine).
- Patients with a high Th1/Th2 ratio were offered the triple therapy LMWH/prednisolone/20% intralipids (100 ml) on day 4-9 of the cycle. Those with a very high Th1/Th2 ratio (>40) were offered this therapy with two intralipid sessions.
Live birth improves after immunotherapy treatment
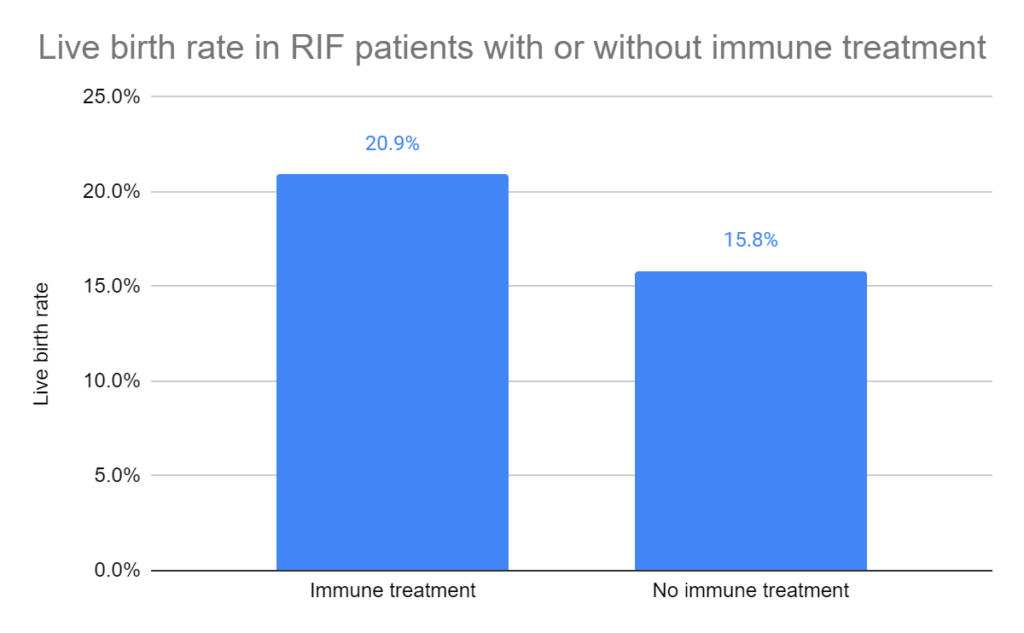
Overall, the live birth increased in immunological RIF patients that had immunotherapy vs those who didn’t (20.9% vs 15.8%, p< 0.001). This was the study’s primary outcome.
Improved pregnancy outcomes after immunotherapy
Besides the overall live birth, they also looked at a number of different pregnancy outcomes after immunotherapy.
They looked at live births for each transfer cycle, up to the 7th transfer and above, which were all statistically significant.
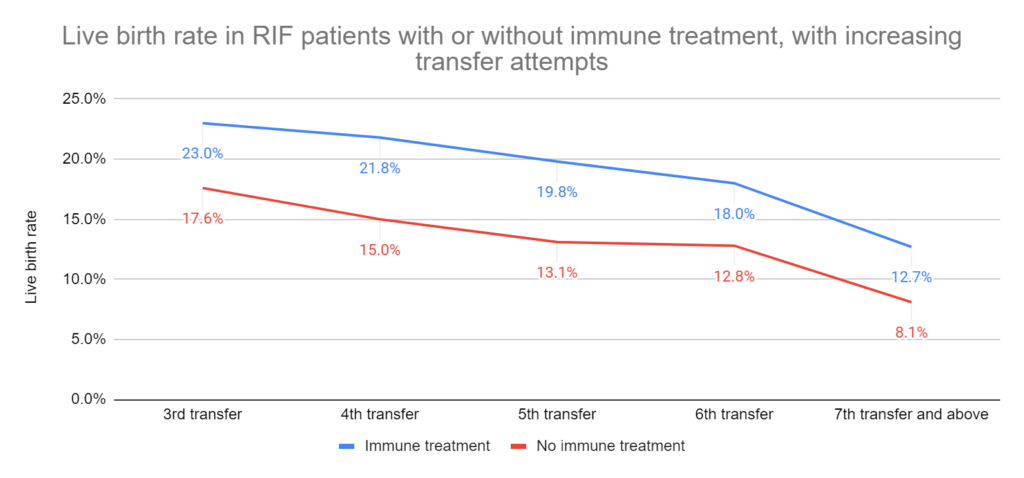
The cumulative live birth rate (up to the 6th cycle) was also higher in patients who had the immune treatment vs those who didn’t (52.9% vs 38.7%, p< 0.001).
They also looked at miscarriage rates (including both biochemical pregnancy losses and clinical miscarriages). There was a higher chance of miscarriage with immune treatment vs no immune treatment (18.6% vs 16.6%, p< 0.01). Another analysis showed that this was related to biochemical losses, and not clinical miscarriages. There were no differences in miscarriage rates in patients transferring a euploid embryo.
Subgroup analysis shows a benefit for immunotherapies
Everything that we’ve seen so far is a mix of all the different patients, including fresh/frozen embryo transfers or triple/dual/single immunotherapy treatments. They did a subgroup analysis to isolate and compare these groups (below, the stats given are live birth rates for immune treatment vs no immune treatment):
- Own eggs: 18.7% vs 14.3%, p< 0.001.
- Donor eggs: 37.25% vs 27.3%, p< 0.001.
- Fresh transfers: 22.2% vs 16.1%, p< 0.001.
- Frozen transfers: 17.9% vs 13.4%, p< 0.01.
- Blastocyst stage frozen transfer: 20.5% vs 16.6%, p< 0.01.
- Triple/dual/single immunotherapy: 25.2%/21.8%/20.1% vs 15.8%, p< 0.001. For miscarriage rates, there were no differences (19.3%/19.7%/17.7% vs 16.6%).
Adjusted statistical models show a benefit for immunotherapies
In a separate analysis (univariate and multivariate regression), they used statistical models to predict live birth after using immune treatments (with statistical adjustment of confounders), and found:
- The use of a single immunotherapy increased the odds of live birth by 37% (adjusted odds ratio [95% CI]: 1.37 [1.21-1.56]). Prednisolone alone increased the odds of live birth by 28%; intralipids alone didn’t increase the odds of live birth; LMWH alone increased the odds of live birth by 37%.
- The use of the dual immunotherapy increased the odds of live birth by 64% (adjusted odds ratio [95% CI]: 1.64 [1.42-1.90]).
- The use of the triple immunotherapy increased the odds of live birth by 97% (adjusted odds ratio [95% CI]: 1.97 [1.70-2.20]).
In yet another analysis (Cox model), they looked at the chance of cumulative live birth over the study period (~20 years):
- The use of immunotherapy increased the hazard ratio (ie. chance) of live birth by 78% (adjusted hazard ratio [95% CI]: 1.78 [1.62–1.94]).
- For triple/dual/single immunotherapies, the hazard ratio for live births increased by 130%/63%/59%.
- For prednisolone/LMWH/intralipids, the hazard ratio for live births increased by 57%/72%/37%.
Conclusions
Overall, this study found that immunological RIF patients had a slight improved live birth rate after using immunotherapies during IVF.
Live births were increased in every subgroup they looked at. The greatest improvement in live birth was when patients used the triple immunotherapy.
Immunotherapies also led to improvements in cumulative live births, along with a slight increase in miscarriages that was related to biochemical losses rather than clinical losses.
The strengths of this study include:
- It’s multicenter and involved 15 IVF clinics in the UK.
- Large number of patients.
- These clinics used a standardized test for evaluating immunological problems.
- The clinics used standardized immune protocols to treat the patients.
- Multiple analyses showed a benefit of immunotherapy (live births, live births by cycle number, cumulative live birth, the various subgroup analyses, different statistical models).
The limitations of this study include:
- It’s retrospective and not an RCT.
- The control group consisted of women who declined immunological testing or tested negative. It would have been much better to include women who tested positive and didn’t receive immunotherapy.
- Most treatments involved multiple immunotherapies. They did show results for single treatment, but provided no information on how large the sample size was for this.
- Although the immunological tests and treatments were standardized between the clinics, there is no universally accepted standard. Without strict criteria for immunological RIF, patients with a wide range of diagnoses were accepted into this study. This could result in over-diagnosis of immunological RIF and over-treatment of patients, which could dilute the results. In other words, if there were better diagnosis criteria for immunological RIF then there might have been a larger impact on live birth rates.
- Uterine NK cells appear to have mostly a supportive role for implantation and it’s not clear how peripheral NK cells tie into this. Read more about this here.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (7 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 RCT finds no benefit for prednisone use among RIF patients
RCT finds no benefit for prednisone use among RIF patients
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Meta-analysis finds no difference in pregnancy outcomes when using the ERA
Meta-analysis finds no difference in pregnancy outcomes when using the ERA
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer
 Increases in immune cells associated with reduced risk of miscarriage
Increases in immune cells associated with reduced risk of miscarriage
 Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies