Researchers in a 2023 study conducted a survey and found that most US clinics have an age policy for providing IVF treatment, with maternal risks of pregnancy as the leading concern.
Fertility treatment is often denied based on age due to higher risks for both the mother and baby, as well as potential health concerns related to advanced paternal age.
Selter et al. (2023) conducted a survey that addressed policies of IVF clinics on patient age and fertility treatment in the US. A total of 366 surveys were sent out to clinics, along with two reminders, of which 69 replied (18.9% response rate).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Most US clinics have an age policy for receiving IVF treatment
Most clinics (88.4%) had a policy for age and fertility treatment:
- 73.9% reported a maximum maternal age for autologous cycles, with an median age of 45 (range 42-54).
- 79.7% reported a maximum maternal age for donor egg cycles, with a median age of 52 (range 48-56).
- 4.3% reported a maximum paternal age, with a median age of 55 (range 55-70).
Maternal risks of pregnancy is the top cited reason for denying fertility treatment
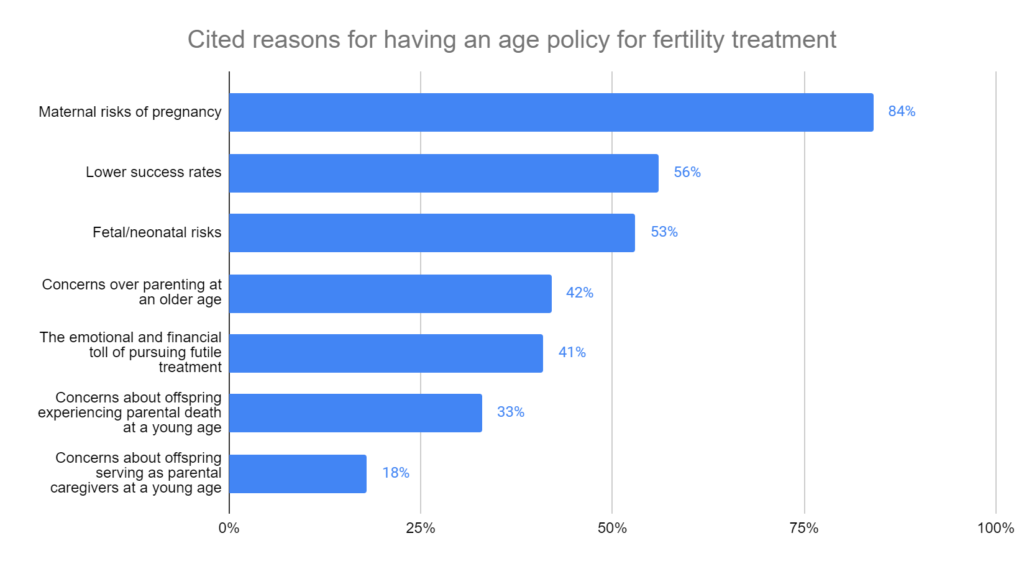
The clinics were asked what their top 3 reasons were for their age policy, which included maternal risks of pregnancy, fetal/neonatal risks, concerns over parenting at an older age, the emotional and financial toll of pursuing futile treatment, concerns about offspring experiencing parental death at a young age, and concerns about offspring serving as parental caregivers at a young age.
The top 3 reasons were maternal risks of pregnancy, lower success rates and fetal/neonatal risks.
Most clinics (55%) granted exceptions for their policies on maternal age:
- 69% for pre-existing embryos.
- 55% for the absence of risk factors for complications in pregnancy.
- 40% for prior uncomplicated pregnancies.
Most clinics want an ASRM policy on maximum maternal age
Most clinics (71%) believe that there should be an American Society of Reproductive Medicine (ASRM) policy for maximum maternal age, with the median maximum as 45 (range 43-54) for autologous cycles, and 51 (range 44-56) for donor cycles.
Conclusions
The majority of clinics had a maternal age policy for fertility treatment, with a median age of 45 for autologous cycles and 52 for donor egg cycles.
The top three reasons for having a maternal age policy were maternal risks of pregnancy, lower success rates and fetal/neonatal risks. Many clinics would make exceptions, particularly for pre-existing embryos.
Very few had a maximum paternal age policy, despite some evidence showing reduced IVF success and potential neurodevelopmental risks in children with advanced paternal age. The authors note that the absence of paternal age policies may be influenced by biases or cultural factors, and that maternal age policies mostly consider pregnancy-related risks that are specific to women.
The inconsistency in clinic policy on age and fertility treatment leads to confusion among patients and puts pressure on providers to offer care in situations where they may not feel comfortable, the authors write. Because of this, most clinics would like ASRM guidance on the topic.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Egg freezing and thawing
Egg freezing and thawing
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 IVF and pregnancy outcomes for women 45+
IVF and pregnancy outcomes for women 45+
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Study finds poor ovarian responders have no further live births after 4 cycles
Study finds poor ovarian responders have no further live births after 4 cycles
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Examining live birth rates in IVF cycles with 5 or less follicles
Examining live birth rates in IVF cycles with 5 or less follicles