A 2026 study found that switching frozen embryo transfer protocols after a failed transfer did not improve live birth compared with repeating the same protocol, including in PGT-A cycles, with some small and uncertain differences seen in specific natural FET types.
After an unsuccessful frozen embryo transfer (FET), many clinics change the FET protocol for the next transfer, often switching between a medicated (programmed) and a natural cycle.
However, it’s not clear which FET protocol is superior, and whether switching from one to another can improve outcomes after an unsuccessful FET.
To address this, Chae-Kim et al. (2026) tested whether changing the FET protocol after an initial unsuccessful FET improves live birth compared with repeating the same protocol.
For more background on FET protocols, check my post Comparing frozen embryo transfer/FET protocols.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: Retrospective study conducted across 4 US-based private fertility practices between 2012 and 2022.
- Participants: 17,989 FET cycles that had a previous failed FET, where patients either repeated the same FET protocol or switched protocols:
- There were four groups: 8,135 repeat medicated FETs; 5,432 repeat natural FETs; 2,206 failed medicated FETs that switched to natural; and 2,225 failed natural FETs that switched to medicated. The average patient age was about 37.
- Exclusions: Recurrent implantation failure, recurrent pregnancy loss, untreated uterine factor infertility or hydrosalpinx, anovulation or PCOS, donor oocytes.
- Embryos: Single blastocyst transfers only; poor-quality embryos below BB were excluded. About half of cycles involved PGT-A.
- Primary outcome: Live birth.
Switching FET protocols after a failed transfer did not improve live birth
The researchers grouped patients based on whether they repeated the same FET protocol for their second frozen embryo transfer or switched protocols after an initial failure. There were four groups:
- Medicated (first failed FET) → medicated (second FET)
- Medicated → natural
- Natural → natural
- Natural → medicated
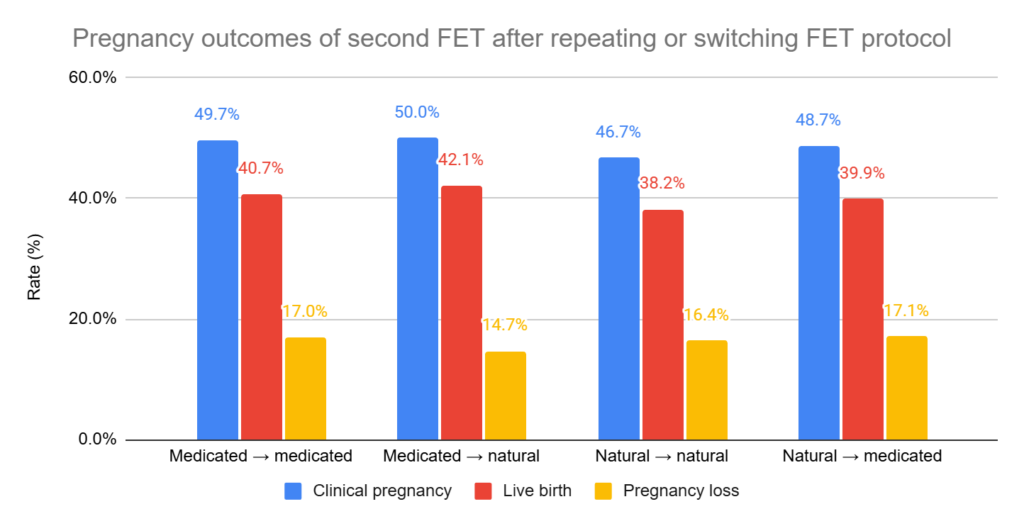
- After a failed medicated FET: Live birth was similar whether patients switched to a natural cycle or repeated a medicated cycle (42.1% vs 40.7%, adjusted relative risk [95% CI]: 1.02 [0.97–1.08]).
- After a failed natural FET: Live birth was also similar whether patients switched to a medicated cycle or repeated a natural cycle (39.9% vs 38.2%, adjusted relative risk [95% CI]: 1.06 [1.00–1.13]).
- There were no statistical differences for clinical pregnancy or pregnancy loss.
About half of these FETs involved PGT-A. When they looked at only PGT-A cycles, there was also no difference (live birth rates ranged from 42.8% to 45.6%).
Outcomes after switching to specific types of natural FET
The results above include all types of natural FET protocols combined. This study included 3 types of natural FET:
- True natural (no ovarian stimulation or trigger)
- Stimulated natural (had ovarian stimulation)
- Modified natural (had a trigger)
The researchers then performed a separate analysis comparing patients who repeated the same approach with those who switched to a specific type of natural FET (8 groups). Note that the “natural” group here includes all subtypes together.
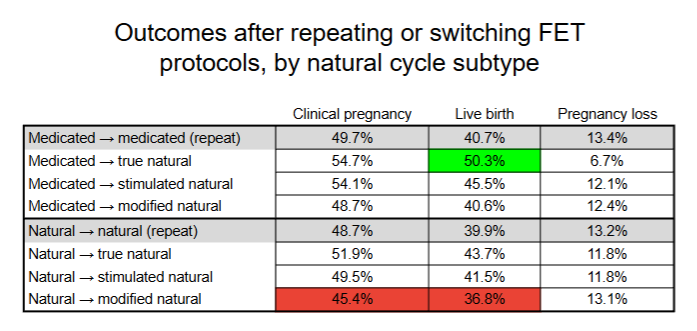
- After a failed medicated FET, switching to a true natural FET: Higher live birth rate compared with repeating a medicated cycle (50.3% vs 40.7%, adjusted relative risk [95% CI]: 1.20 [1.03–1.39]).
- After a failed natural FET, switching to a modified natural FET: Lower live birth rate compared with repeating a natural cycle (36.8% vs 39.9%, adjusted relative risk [95% CI]: 0.91 [0.85–0.97]). Also lower clinical pregnancy.
- There were no other statistically significant differences.
Conclusion
This study found that switching frozen embryo transfer protocols after a failed transfer did not improve live birth rates compared with repeating the same protocol. This was true whether patients switched from medicated to natural cycles or from natural to medicated cycles, and it was also true when only PGT-A cycles were analyzed.
When natural cycles were broken down into subtypes, most comparisons still showed no difference. Switching from a failed medicated cycle to a true natural cycle was linked to a higher live birth rate, while switching from a failed natural cycle to a modified natural cycle was linked to lower live birth and clinical pregnancy rates.
The authors explain that the differences in the natural FET subtype analysis may be due to lower pregnancy loss, selection bias from cancelled cycles in true natural FETs, or chance, and should not be overinterpreted without confirmation in future studies.
Limitations include the retrospective design, limited detail on why FET protocols were chosen or changed, exclusion of some patient groups (anovulatory patients), and the lack of adverse pregnancy outcome data (which is relevant because other studies have reported higher rates of preeclampsia with medicated FET cycles).
Want to read more about FET protocols?

The post discusses various frozen embryo transfer protocols, which includes a medicated FET, natural cycle FET (true natural/modified natural), and mild ovarian stimulated FET, along with their scheduling. In addition, it examines whether one FET protocol is superior to another, the relevance of the corpus luteum in medicated vs natural cycle FETs, and optimal progesterone levels. Read more.

A 2025 randomized controlled trial found that natural cycle FETs led to higher live birth rates and fewer miscarriages than medicated FETs in ovulatory women with a good prognosis. Read more.

Researchers in a 2023 study found decreased adverse pregnancy and neonatal outcomes in those who performed a natural vs medicated FET, including abnormal birth weights, preeclampsia, preterm births, and more. Read more.
Researchers in a 2023 study share the results of a survey that evaluates the use and attitude of natural cycle FETs in US clinics, which some studies have recently shown can lead to improved pregnancy outcomes compared to medicated FETs. Read more.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.