A 2026 study found that if endometrial fluid cleared before embryo transfer, live birth rates were similar to patients without fluid. When the fluid remained, live birth rates were lower, and cancelling the cycle didn’t appear to improve outcomes in a later transfer.
Even when euploids are transferred, implantation is not guaranteed, which means that uterine factors still matter.
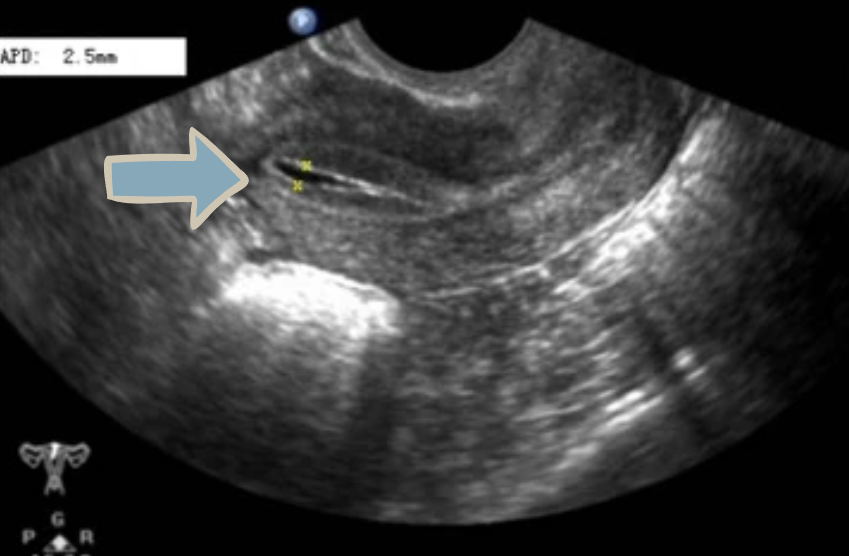
One issue that sometimes comes up during a frozen embryo transfer (FET) cycle is endometrial fluid. This is fluid seen inside the uterine cavity and might come from mucus, blood, inflammatory secretions, or fluid from the fallopian tubes. Doctors usually detect it during transvaginal ultrasound monitoring while the uterine lining is thickening under estrogen, before progesterone is started.
Some studies have found that endometrial fluid is linked to lower pregnancy rates. Because of this, some clinics cancel transfers when fluid is present, while others might proceed if the fluid resolves and disappears on ultrasound. It’s unclear whether waiting for the fluid to resolve actually improves success rates.
Another limitation is that many earlier studies included untested embryos, making it hard to know whether poorer outcomes were caused by the embryo or the uterus.
A study by Patel et al. (2026) compared outcomes for patients with or without endometrial fluid who transferred a single euploid embryo. The researchers also examined what happened when transfers were cancelled because of fluid and patients returned for another transfer later.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: Retrospective study conducted at a single fertility center in the US between 2014 and 2022.
-
Participants: 4308 patients (average age 35-36) undergoing their first FET after their first IVF cycle with PGT-A and at least one euploid embryo. Cycles were grouped based on the presence of endometrial fluid seen on ultrasound.
- No endometrial fluid (control, 4104 patients): No fluid was detected during monitoring.
- Fluid resolved (108 patients): Fluid was seen during monitoring but disappeared before progesterone start or ovulation trigger.
- Fluid persisted (60 patients): Fluid was still present on ultrasound on the day on progesterone start or ovulation trigger.
- Embryos transferred: Mostly day 5 or 6 euploids graded 3BB or higher.
- FET protocols: Patients underwent natural, modified natural, or medicated FETs.
- Primary outcome: Live birth rate per embryo transfer.
Persistent endometrial fluid was linked to lower live birth
Endometrial fluid was detected during ultrasound monitoring in 168 of the 4308 patients (3.9%) before transfer. By the time progesterone was started or ovulation was triggered, the fluid had either resolved or was still present, and transfer outcomes were measured.
- No fluid: live birth rate 58.5%
- Fluid resolved: 49.1% (no difference compared to patients with no fluid, adjusted odds ratio [95% CI]: 0.71 [0.47–1.05])
- Fluid persisted: 38.3% (lower compared to patients with no fluid, adjusted odds ratio [95% CI]: 0.50 [0.28-0.88])
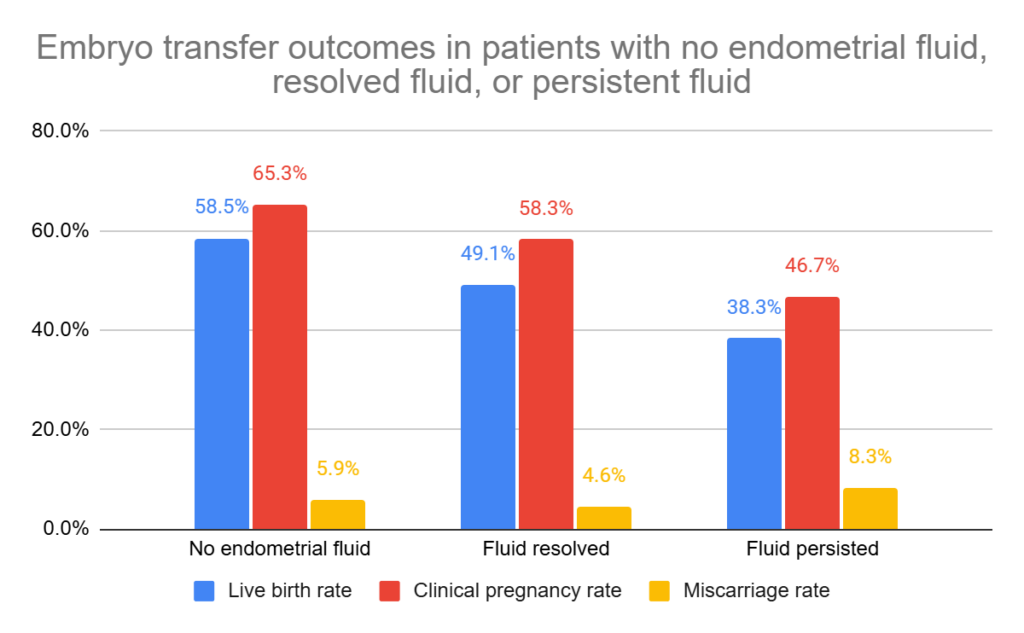
There were no statistically significant differences in miscarriage rates between the groups.
Among the 60 patients with persistent endometrial fluid, 14 had a repeat ultrasound showing the fluid resolved (live birth rate 28.6%) while the remaining 46 did not have a follow-up scan (live birth rate 41.4%), with no significant difference between groups. Two patients had the fluid aspirated before transfer and neither became pregnant.
Cancelling a cycle due to endometrial fluid didn’t improve live birth in the next transfer
Separate from the analysis above, the authors examined 58 cycles that were cancelled due to endometrial fluid and went on to have another transfer. This group was small so it’s hard to make meaningful comparisons, but below is an overview of how many patients were in each group:
- 58 had endometrial fluid and cancelled their first transfer, then went on to have a subsequent completed transfer
- 35 showed no endometrial fluid at transfer
- 23 showed endometrial fluid again at transfer
- 9 had the fluid resolve before progesterone start
- 14 had the fluid persist at progesterone start
Of the 58 patients who had another transfer, the overall live birth rate was 39.7%. This was similar to the 38.3% live birth rate in patients who had persistent fluid from the original cohort. In other words, cancelling the cycle didn’t appear to improve live birth rates to the level seen in patients who never had fluid.
It’s important to note that the authors grouped all 58 later transfers together, whether endometrial fluid was present again or not. This means the results show what happens after cancelling and trying again later, rather than whether cancelling helps when the fluid actually resolves.
Conclusion
This study showed that when endometrial fluid resolved before progesterone/trigger, live birth rates were slightly lower but not significantly different, suggesting it’s still reasonable to proceed with a transfer.
When fluid persisted, live birth rates were lower. Cancelling the cycle and transferring later didn’t change the chance of live birth.
Fluid in the uterine cavity could interfere with implantation through several mechanisms, such as physically displacing the embryo or inflammation, although this study didn’t directly examine these factors. One observation was that the endometrial fluid group was enriched in patients with a history of cesarean section, suggesting that scarring or altered uterine architecture might contribute to fluid accumulation.
The authors noted that many patients had fluid appear again in later cycles and some required multiple transfers to achieve a live birth, suggesting that persistent fluid may reflect underlying patient factors affecting the uterine environment and not just a single cycle issue.
Limitations include the retrospective single center design, small sample sizes in the endometrial fluid groups, unknown causes and inconsistent measurement of the fluid, and inclusion of different FET protocols.
Want to read more about the uterine environment and success rates?
A large 2025 study found that a thin lining (<7 mm) lowered live birth rates in medicated and modified natural FETs, but not in natural cycles, and overall endometrial thickness was not a strong standalone predictor of IVF success. Read more.
A 2024 study combined the results of 14 studies analyzing how hysteroscopy impacts IVF success, finding improvements in live birth rate, pregnancy rate and no change in miscarriage rate. Read more.
A new study reviewed how fibroids can compromise the endometrium and prevent embryo implantation, identifying key issues such as disrupted blood flow and vascular changes, abnormal endometrial peristalsis, inflammatory responses, and changes in the microbiome. Read more.
Related studies
These are additional studies that haven’t been covered on Remembryo. They may be helpful if you’re exploring this topic further. This section is available for paid subscribers.

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.