
Researchers in a 2022 study performed a meta-analysis to combine the results of studies examining the transfer of a good and poor quality embryo together (vs one good quality embryo alone), and found no differences in pregnancy or live birth rates, but increases in the rate of multiples.
Many IVF patients combine good and poor quality embryos together for a transfer, and some studies have found that this can be detrimental and can lead to reduced success rates. This might be due to the endometrium sensing poor quality embryos that can lead to inhibition of implantation.
Xiao et al. (2022), in their systematic review and meta-analysis, pooled the results of 17 studies that examined outcomes from the transfer of a single good quality embryo (17,612 cycles) compared to the transfer of both a good and poor quality embryo together (6,431 cycles). The included studies were current to 2021.
Check out my complete guide to embryo grading and success rates to learn more about embryo development, grading and success rates.
One major limitation of this study, in my opinion, is that it didn’t differentiate between Day 5, 6, and 7 blastocysts. While Day 7 transfers are generally rare, Day 5 embryos tend to have higher implantation potential than Day 6. Given the large sample size, this may have balanced out overall. However, the fresh blastocyst transfer data likely involved only Day 5 embryos, making those results somewhat more reliable.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
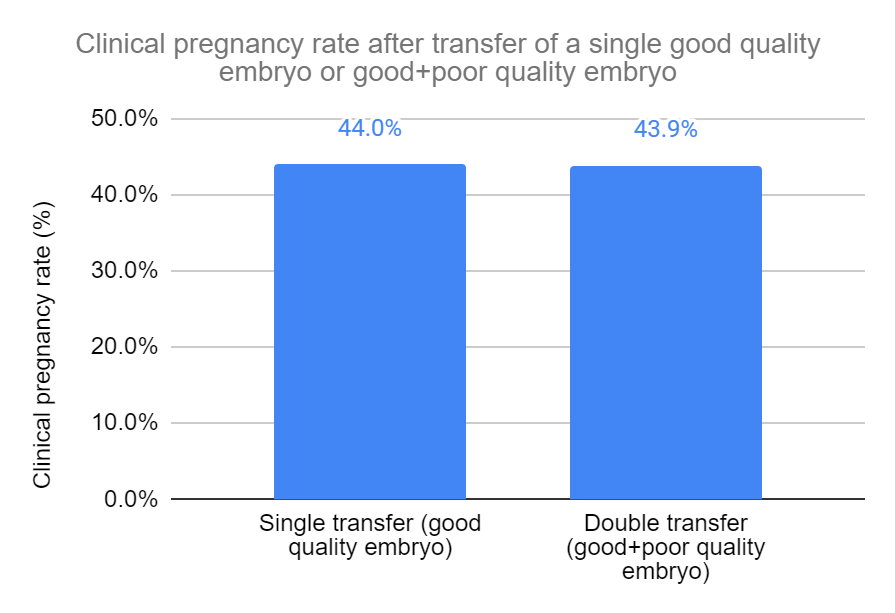
No difference in clinical pregnancies when transferring a good and poor quality embryo together
Based on 15 studies and 14,605 participants, there was no statistically significant difference in clinical pregnancy rates in women who transferred a single good quality embryo vs a transfer of both a good and poor quality embryo (44.0% vs 43.9%, risk ratio [95% CI]: 1.02 [0.91-1.14]). There was significant heterogeneity (I2 = 79%).
This data from the 15 studies included fresh, frozen, blastocyst and cleavage stage embryo transfers. So they split up these groups in a subgroup analysis to see the individual impact on clinical pregnancy rates.
Fresh cleavage stage embryos
Based on 5 studies and 7,538 participants, there was no statistically significant difference in clinical pregnancy rates in women who transferred a single fresh good quality cleavage stage embryo vs a fresh transfer of both a good and poor quality cleavage stage embryo (41.8% vs 36.0%, risk ratio [95% CI]: 1.02 [0.71-1.45]). There was significant heterogeneity (I2 = 92%).
Fresh blastocyst transfers
Based on 6 studies and 3,198 participants, there was no statistically significant difference in clinical pregnancy rates in women who transferred a single fresh good quality blastocyst vs a fresh transfer of both a good and poor quality blastocyst (52.8% vs 50.8%, risk ratio [95% CI]: 1.05 [0.97-1.14]).
Frozen blastocyst transfers
Based on 4 studies and 2,781 participants, there was no statistically significant difference in clinical pregnancy rates in women who transferred a single frozen good quality blastocyst vs a frozen transfer of both a good and poor quality blastocyst (43.7% vs 50.0%, risk ratio [95% CI]: 0.97 [0.83-1.15]). There was significant heterogeneity (I2 = 67%).
Blastocyst quality ≥3BB and <3BB
Between the 15 studies, there were inconsistencies in how embryos were graded as good or poor quality. To get around this, they did another subgroup analysis using only studies that defined good quality blastocysts as ≥3BB and poor quality blastocysts as <3BB. Check my post on embryo grading to make sense of this if you’re unclear.
Based on 5 studies and 3,901 participants, there was no statistically significant difference in clinical pregnancy rates in women who transferred a single good quality blastocyst (≥3BB) vs a transfer of both a good (≥3BB) and poor quality (<3BB) blastocyst (42.6% vs 48.0%, risk ratio [95% CI]: 1.03 [0.86-1.23]). There was significant heterogeneity (I2 = 73%).
Increase in multiple pregnancy rate when transferring good and poor quality embryos together
Transferring more than one embryo is often discouraged due to the risk of multiples.
Based on 13 studies and 5,355 participants, there was a statistically significant decrease in multiple pregnancy rates in women who transferred a good quality embryo vs transfer of both a good and poor quality embryo (1.7% vs 21.6%, risk ratio [95% CI]: 0.14 [0.09-0.20]). This means that women who transferred the two embryos were about 7 times more likely to have a multiple pregnancy.

They performed a subgroup analysis as before and found that multiple pregnancy rates increased for each group (all statistically significant):
- Fresh cleavage stage embryos (4 studies, 2,816 participants, 1.5% vs 7.6%)
- Fresh blastocyst (5 studies, 788 participants, 2.5% vs 22.6%)
- Frozen blastocyst (4 studies, 1,288 participants, 1.8% vs 26.4%)
- Blastocyst quality ≥3BB and <3BB (5 studies, 1,733 participants, 2.2% vs 26.0%)
No difference in live birth rates when transferring a good and poor quality embryo together
Based on 11 studies and 17,269 participants, there was no statistically significant difference in live birth rates in women who transferred a single good quality embryo vs transfer of both a good and poor quality embryo (36.8% vs 39.8%, risk ratio [95% CI]: 0.96 [0.87-1.07]). There was significant heterogeneity (I2 = 79%).

They performed a subgroup analysis as before and found that there were no differences in live birth rates for each group:
- Fresh cleavage stage embryos (2 studies, 1,832 participants, 25.0% vs 28.2%)
- Fresh blastocyst (5 studies, 6,842 participants, 43.5% vs 46.2%)
- Frozen blastocyst (4 studies, 3,259 participants, 40.0% vs 43.7%)
- Blastocyst quality ≥3BB and <3BB (5 studies, 4,379 participants, 37.4% vs 41.9%)
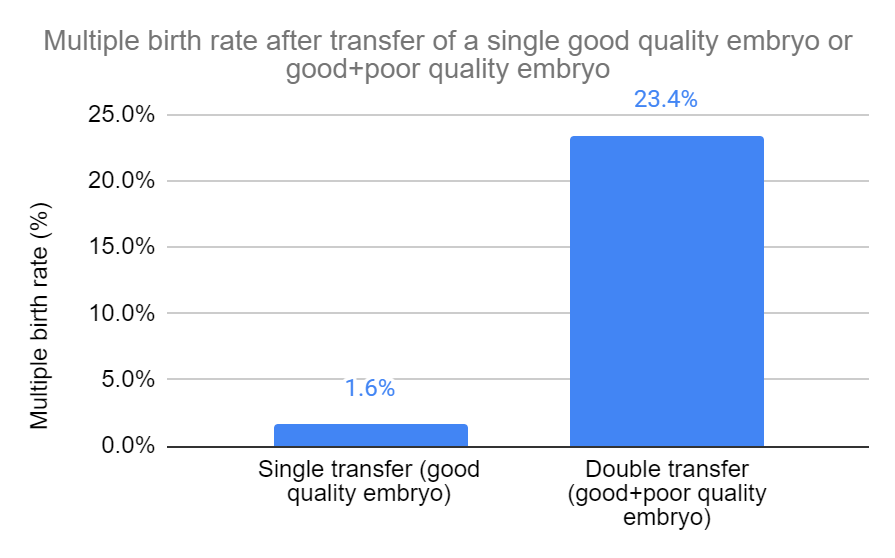
Increase in multiple birth rate when transferring good and poor quality embryos together
Based on 6 studies and 5,050 participants, there was a statistically significant decrease in multiple birth rates in women who transferred a single good quality embryo vs transfer of both a good and poor quality embryo (1.6% vs 23.4%, risk ratio [95% CI]: 0.08 [0.06-0.12]). This means that women who transferred the two embryos were about 12 times more likely to have a multiple pregnancy.
They performed a subgroup analysis as before and found that multiple birth rates increased for each group (all statistically significant):
- Fresh cleavage stage embryos (3 studies, 2,563 participants, 1.4% vs 27.4%)
- Fresh blastocyst (3 studies, 893 participants, 2.4% vs 30.6%)
- Blastocyst quality ≥3BB and <3BB (3 studies, 999 participants, 2.7% vs 29.9%)
Conclusions
This study found no differences in clinical pregnancy or live birth rates when transferring a single good quality embryo or both a good and poor quality embryo together.
Multiple pregnancy and live birth rates increased when transferring both good and poor quality embryos together compared to just a single good quality embryo.
The authors state that patients with good and poor quality embryos should consider transferring a single good quality embryo rather than combining it with a poor quality embryo. This study found no benefit in transferring a good and poor quality embryo together, but instead shows an increase in the rate of multiples. However the authors acknowledge the stress associated with going through a second transfer and think this should be considered for some patients.
As mentioned earlier, a major limitation is not differentiating between day 5, 6 and 7. The authors also noted that there was considerable heterogeneity in the studies. This was because of differences in how embryos are evaluated as good/poor, particularly for cleavage stage embryos.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Study examines transferring a good and poor quality embryo together
Study examines transferring a good and poor quality embryo together
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Grade C (poor quality) embryo success rates
Grade C (poor quality) embryo success rates
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation
Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation
 AI model predicts live births from blastocyst images with highest accuracy yet
AI model predicts live births from blastocyst images with highest accuracy yet