
This post takes a closer look at what “poor-quality” embryos really mean in IVF. At the cleavage stage, they often have fewer cells or high fragmentation, while at the blastocyst stage, a grade C means the inner cell mass and trophectoderm contain fewer, loosely packed cells. These embryos tend to have lower success rates than good-quality ones, but studies show they can have similar perinatal outcomes.
This post goes over what makes up a poor quality embryo, but to learn more about embryo grading, check out my complete guide to embryo grading and success rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
What is a poor quality embryo?
Embryos are ranked based on the way they look under the microscope, usually as good, fair and poor. Embryos with a higher quality tend to have a better chance of success after transfer.
Embryos are graded differently depending on their stage, and in this post we’ll be discussing poor quality cleavage stage (days 1-3) and blastocyst stage (days 5+) embryos.

Poor quality cleavage stage embryos
The cleavage stage generally occurs between days 1-3 after insemination, where you can count the individual cells of the embryo.
For cleavage stage embryos, the amount of fragmentation generally dictates an embryo’s quality. Fragmentation is when a piece of a cell pinches off of a cell. This usually happens as the cell is dividing (or “cleaving”), and some divisions may leave behind more fragments than others. You can see some examples of fragmentation in embryo pictures below:

As you can tell, it gets pretty hard to tell where the actual cells are when there’s more fragmentation. In the 10% fragmentation picture, you can see 4 larger cells with a bit of fragmentation toward the top. With the other two pictures that have more fragmentation, it’s harder to count the individual cells. As fragments are lost, the original cell that fragmented gets smaller. Imagine taking a snowball and removing pieces of it – the snowball itself gets smaller as each piece is removed.
Racowsky et al. (2011) show that SART’s parameters (0%, <10%, 10-25%, >25% fragmentation) correlate well with live birth rates. In general, many cleavage stage embryos receive their grade based on the amount of fragmentation:
- Good: <10% fragmentation
- Fair: 10-25% fragmentation
- Poor: >25% fragmentation
Fragmentation is one way to describe an embryo’s quality, and is often used to determine if an embryo is good, fair or poor. However there are other features that can be used to evaluate a cleavage stage embryo’s quality.
The number of cells we see in a cleavage stage embryo on a particular day has to do with how fast those cells are dividing. Typically, embryos with around 8 cells (or more!) on day 3 are considered ideal while embryos with fewer cells are considered lower quality.

Clinics can have different ways of reporting grades. One way is based on two numbers, for example a 1/4:
The first number (1 in this case) is the quality. This refers to the quality of the embryo, or grade, which is based on the % fragmentation:
- 1 (poor quality): >25% fragmentation
- 2 (fair quality): 10-25% fragmentation
- 3 (good quality): 1-10% fragmentation
- 4 (good quality): 0% fragmentation
The second number (4 in this case) is the number of cells. So in a 1/4 there’s 4 cells with >25% fragmentation, and because of the “1” this embryo is poor quality.
There can be “house rules” when it comes to grading the quality of a cleavage stage embryo, which can modify the quality grade number. For example, on day 3 we expect around 8 cells, and having 4 cells or less might be grounds to downgrade an embryo’s quality to a 1, even if the embryo doesn’t have much fragmentation. The idea here is that having such a small number of cells can be as detrimental as having a high amount of fragmentation.
Grade C (poor quality) blastocyst stage embryos
After the cleavage stage (and morula stage), a blastocyst develops. This usually occurs about 5 days after insemination of the egg.
Blastocysts look very different from cleavage stage embryos. At this stage, there are structures called the inner cell mass (ICM) and the trophectoderm. The ICM becomes the fetus and the trophectoderm becomes the placenta. When grading blastocysts, the quality of these two structures is what’s important.
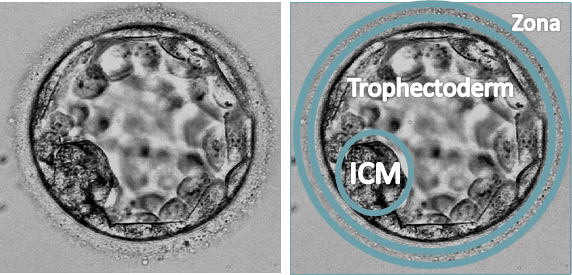
The number of cells that are in these structures, as well as how packed they are, is what determines the grade. A letter is assigned depending on the quality (A=good, B=fair, C=poor). An “A” quality ICM is large and has lots of cells, whereas a “C” quality ICM is small and has a few cells.
A blastocyst is usually given an alphanumeric grade, based on the Gardner system, ie. a 4BA. In this example, the quality of the ICM is the first letter (B), and the quality of the trophectoderm is the second letter (A). The number refers to the “expansion,” and tells us how developed the blastocyst is. The number doesn’t tell us about the quality of the blastocyst.
Below is an image of blastocysts with differently graded ICMs. Notice how much smaller the C grade ICM is and how you can see individual cells, whereas the A grade ICM is larger and more compacted. In the A grade ICM, you can’t really see the individual cells anymore because they’re so compacted.

A separate grade is given to the trophectoderm, and like the ICM, the quality is evaluated by the number of cells and how packed they are. The trophectoderm is essentially all the other cells in the blastocyst besides the ICM.

Together these scores for the ICM and trophectoderm give the overall quality of the blastocyst. A poor quality blastocyst has a C graded ICM or a C graded trophectoderm. Sometimes both of these structures have a C, making it a CC graded embryo.
Poor quality embryo success rates
Embryos are graded to rank them for transfer. Different research has shown that embryos with better grades tend to have a higher chance of implanting and leading to a pregnancy.
So for example, if you have 2 embryos and one has a “good” grade and the other has a “poor” grade, the embryo with the good grade will be transferred first. This is because it’s more likely to lead to a pregnancy than the poorly graded embryo. But this doesn’t mean that a low quality embryo won’t go on to form a pregnancy!
Let’s look at some studies that show how poor quality embryos perform.
Poor quality cleavage stage (day 2-3) success rates
Racowsky (2011) looked at day 3 transfers based on cell number, symmetry and fragmentation. Symmetry has to do with how evenly sized each of the cells are in a cleavage stage embryo.
- 8 cells was ideal with a 25% chance of live birth, <6 cells had the lowest rates at 2.5%
- <10% fragmentation was ideal with 25% birth rate, embryos with >25% fragmentation had a 2.5% chance
- Perfect symmetry was 25% live birth vs 5% with severe asymmetry
Rhenman (2015) looked at day 2 single embryo transfers:
- Having 4 cells was ideal (30% live birth) and dropped to 3-8% with 2-3 cells
- <10% fragmentation was ideal and had a 30% live birth, >50% was about 10%
- The patients average age was 34
Oron (2014) found that live birth rates from poor quality day 2/3 embryos were about half what they are from good quality.
Zhu et al. (2014) compared pregnancy outcomes after transferring 2 good or 2 poor quality day 3 embryos (good quality: 7-8 cells, <10% fragmentation; poor quality: ≤5 cells and/or 30–50% fragmentation):
- Clinical pregnancy was decreased with poor quality embryos (50.26% vs 16.15%).
- Live birth was decreased (39.60% vs 11.41%).
- Miscarriage was increased (13.28% vs 19.77%).
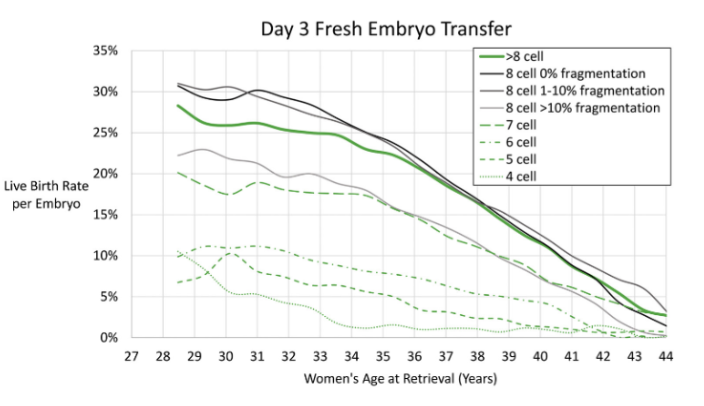
You can see how this all plays out in terms of age, fragmentation and cell number below. This graph, from Awadalla et al. (2022), is based on modeling from US clinic data between 2016-2018. Read more in my post: Predicting live birth rates, multiples based on 223,377 transfers.
How likely a day 3 embryo becomes a blastocyst is also influenced by its quality. Liu et al. (2022) showed that day 3 embryos with ≥20% fragmentation had about a 15% lower chance of forming blastocysts compared to those with less fragmentation. Embryos with fewer than 6 cells had about a 30% chance of reaching the blastocyst stage, compared to 60–80% for those with more cells. Blastocysts that formed from these lower quality day 3 embryos were less likely to lead to a pregnancy. Read more in my post: Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation.
Overall, these studies show that poor quality cleavage stage embryos are less likely to form blastocysts and at least half as effective as good quality embryos in producing a live birth after transfer. Some studies show a more dramatic decrease in success rates. There may be an increased risk of miscarriage with poor quality cleavage stage embryos.
Grade C blastocyst stage (Day 5+) success rates
Zou et al. (2023) compared good, fair and poor quality blastocyst outcomes after a single embryo was transferred. They compared individual grades:
- Good quality live birth rate was 44.4%, miscarriage rate 7.3%
- AC quality: 33.3%
- CA quality: 33.3%
- BC quality: 33.1%, miscarriage rate 10.8%
- CB quality: 24.6%, miscarriage rate 10.5%
- CC quality: 13.7%
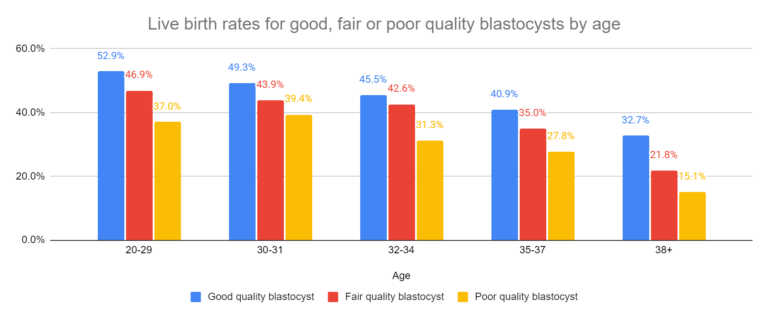
Overall, they found that the odds of live birth with a poor quality embryo was about half that of a good quality embryo. They also looked at how age impacted success rates, finding that age further reduced live birth rates.
Read more in my post: Poor quality blastocysts show acceptable live birth rates, no change in perinatal outcomes.
Bouillon et al. (2017) compared the transfer of a single good, fair or poor quality embryo (good: AA, AB, BA; fair: BB; poor: CC, CB, CA, AC, BC):
- Decrease in clinical pregnancy rates for good vs fair vs poor (55.6% vs 47.2% vs 43.6%).
- Decrease in live birth rates (46.8% vs 39.0% vs 34.1%).
- No statistical difference in miscarriages (13.7% vs 14.6% vs 18.7%).
Van den Abbeel et al. (2013) found a decrease in live birth rates after transferring a single C grade embryo vs an A grade embryo (20% vs 45%) for ages <35.
Oron (2014) looked at single embryo transfers in women <40 years of age, and found that good quality blasts (≥3BB) had a live birth rate of 41% compared to poor quality (<3BB) embryos with a live birth rate of 26%.
Can poor quality embryos still be euploid and lead to success?
Some embryos that look poor under the microscope can still be chromosomally normal (euploid). Do the chances of euploidy decrease in poor quality embryos? And do poor quality euploids have reduced success compared to better quality euploids?
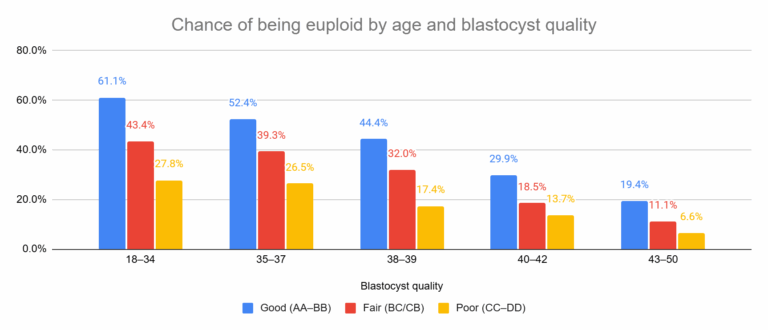
Al Hashimi et al. (2025) found that poor quality blastocysts are less likely to be euploid, and this chance is reduced with age.
They also showed that poor quality euploids can have a higher chance of success compared to untested: transfer of untested poor quality embryos led to live births in about 1 in 10 cases, compared with about 1 in 4 when PGT-A was used. Read more in my post: Poor quality embryos can still lead to live births, especially after PGT-A.
Florensa et al. (2024) also showed a reduced chance of getting a euploid/low level mosaic with poor quality embryos. Read more in my post: Study compares euploid and thaw survival rates of blastocysts biopsied for PGT-A.
In a meta-analysis, Cimadomo et al. (2023) found that poor quality euploid blastocysts had about half the chance of live birth compared to fair or good quality euploids. They also found an increase in miscarriage rate. Read more in my post: Meta-analysis combines 74 studies to examine factors linked to euploid transfer success.
Overall, these studies show that poor quality blastocyst stage embryos are about half as effective as good quality embryos in producing a live birth after transfer, with a possible increased risk of miscarriage.
Do poor quality embryos have a higher chance of pregnancy complications?
For day 3 embryos, Zhu et al. (2014) found no increased risk of stillbirths, ectopic pregnancies, complications, birth weights or other birth outcomes.
For day 5 embryos, Bouillon et al. (2017) found no increased risk of ectopic pregnancies, preeclampsia, preterm birth, low birth weight, neonatal complications or other outcomes. Zou et al. (2023) also showed that there were no differences in preterm birth rates, birthweights, or perinatal outcomes.
In terms of birth defects, Bouillon et al. (2017) and Du et al. (2025) both found no differences for good quality vs poor quality embryos. Other studies, like Abel et al. (2019), have found increased birth defects, but it’s not clear if this is related to the reduced chance of euploidy. Studying this is difficult because of how rare these defects are. Read more in my post: Don’t fear the C-grade: Study finds no higher risk of birth defects with poor-quality embryos.
In their review of 27 articles, Kemper et al (2021) concluded that low quality embryos had “no adverse effects on perinatal outcomes,” although they note that there isn’t much data and higher quality studies are needed.
Why do clinics discard poor quality embryos?
Policies on transferring lower-graded embryos can vary between clinics and some clinics will not transfer these embryos or perform biopsies on them for PGT-A. This is usually influenced by different laboratory grading thresholds, internal clinic policies, and the doctor’s decision.
On average, these embryos have reduced implantation rates and higher risks of miscarriage compared with higher graded embryos. Because of this, some clinics have minimum quality thresholds for transfer and will discard embryos that don’t meet this threshold.
However, these thresholds aren’t always clearly defined, and many studies group all “poor quality” embryos together, even though outcomes can vary across different grades (Kemper et al. 2021).
According to Kemper et al. 2021, clinics may avoid using lower quality embryos because success rates are usually reported per transfer, so selecting only the best embryos can improve reported outcomes and make the clinic appear more competitive.
We advocate that [lower quality embryos] not be universally discarded, but rather be considered for transfer in conjunction with the patient’s personalized treatment plan.
Conclusions
An embryo’s quality depends on certain features that you can see under the microscope. These features are different depending on whether the embryo is a cleavage stage embryo (day 3) or a blastocyst (day 5+).
Cleavage stage embryos are primarily evaluated based on the number of cells they have and the amount of fragmentation. Embryos with a lot of fragmentation have a lower quality.
Blastocyst stage embryos are evaluated based on how many cells there are in the inner cell mass (ICM) and trophectoderm. Blastocysts with few cells in their ICM or trophectoderm are poor quality.
Studies have shown that poor quality embryos have about half the chance of success as a good quality embryo, although this is sometimes higher (or lower) depending on the study.
There might be an increased chance of miscarriage, but there doesn’t seem to be any increases in adverse pregnancy or perinatal outcomes.
Clinics might discard these embryos as part of their policy. Although the chances may be lower, they’re not zero, and in the right context these embryos are worth considering.
💡 Want to see real success stories with lower-grade embryos?
Check the IVF Success: Poor quality embryo collection from the Uterine Wall of Fame, which features a growing collection of IVF success stories submitted by people who have been through it themselves.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Transferring a good and poor quality embryo together: a meta-analysis
Transferring a good and poor quality embryo together: a meta-analysis
 Predicting how many day 3 embryos make it to blastocyst
Predicting how many day 3 embryos make it to blastocyst
 AI model predicts live births from blastocyst images with highest accuracy yet
AI model predicts live births from blastocyst images with highest accuracy yet
 Study examines association with embryo quality and male to female sex ratio
Study examines association with embryo quality and male to female sex ratio
 Study evaluates the potential of day 4, 5, 6 and 7 blastocysts
Study evaluates the potential of day 4, 5, 6 and 7 blastocysts