Researchers in a 2022 study found improved pregnancy outcomes using letrozole-stimulated FETs compared to medicated FETs, which were comparable to natural FETs.
There are a number of options for endometrial preparation for a frozen embryo transfer (FET), including a medicated or a natural FET, as well as an FET following mild ovarian stimulation. Check out my post on the different FET protocols to learn more about them.
Godiwala et al. (2022), in their retrospective study, compared pregnancy outcomes of different FET protocols at a single center in the US between 2015 and 2021. They looked at medicated FETs (1,407 cycles), true natural FETs (1,450 cycles) and FET following ovarian stimulation with letrozole (from here on “letrozole FETs,” 291 cycles).
No trigger was used in natural or letrozole FETs and luteinizing hormone (LH) surge was monitored for ovulation.
There were a number of differences (“confounders”) between the baseline patient and cycle characteristics, particularly in patient age, BMI, AMH levels, number of embryos transferred and number of previous IVF cycles. These factors can change the results, however these were all accounted for and controlled in their statistical analysis.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Live birth rates were highest with letrozole and natural cycle FETs
Ongoing pregnancies and live birth rates were combined in this study as a single outcome. Ongoing pregnancies were defined as a viable pregnancy beyond 10 weeks.
Women who had a letrozole-FET (63.6%) had a significantly higher ongoing pregnancy and live birth rate compared to medicated FETs (55.7%).

After statistical adjustment there was still a significant increase (adjusted relative risk [95% CI]: 1.11 [1.02-1.21]). This means that after accounting for the different confounders (age, BMI, etc. which might be influencing the data), there was still an increase of 11% – so if a medicated FET had a ongoing pregnancy/live birth rate of 50%, then a letrozole FET would be 55.5% (11% increase from 50%).
There were no statistical differences between natural FETs and medicated FETs, or between natural FETs and letrozole FETs.
Miscarriage rates were lowest with natural FETs
There was a significant decrease in miscarriage rates between natural FETs (10.1%) and medicated FETs (17.2%).
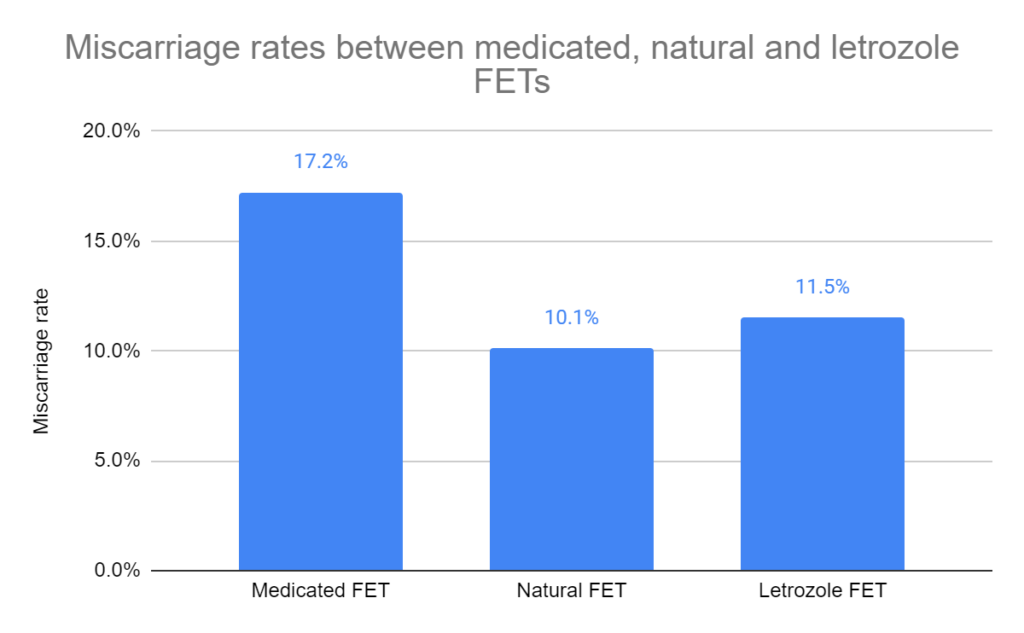
After statistical adjustment, there was still a significant decrease (adjusted relative risk [95% CI]: 0.62 [0.46-0.84]). This means that after accounting for the different confounders (age, BMI, etc. which might be influencing the data), there was still a decrease of 38% (1.00-0.62=0.38) – so if a medicated FET had a miscarriage rate of 10%, then a natural FET would be 6.2% (38% increase from 10%).
There were no statistically significant differences in miscarriage rates between letrozole FETs and medicated FETs or natural FETs.
In ovulatory women, letrozole FETs had the highest live birth rates
A subgroup analysis was performed where they compared outcomes from women that ovulated normally and those who didn’t (who were anovulatory or had PCOS).
Ovulatory women showed higher ongoing pregnancies and live birth rates when performing a letrozole FET (67.0%) compared to a medicated FET (55.1%).

This was still significant after statistical adjustment (adjusted relative risk [95% CI]: 1.16 [1.05-1.28]). This means that after accounting for the different confounders (age, BMI, etc. which might be influencing the data), there was still a increase of 16% – so if a medicated FET had an ongoing pregnancy/live birth rate of 50%, then a letrozole FET would be 58% (16% increase from 50%).
There was no difference in ongoing pregnancies and live birth rates between natural FETs and letrozole or medicated FETs.
No difference in letrozole or medicated FET protocols among anovulatory/PCOS women
In a subgroup analysis that compared women who were anovulatory or had PCOS, there were no differences in ongoing pregnancy or live birth rates between medicated and letrozole FET protocols. There were also no differences in miscarriage rates.
The authors note that these results may be due to the smaller sample size.
Conclusions
In this study they found increased ongoing pregnancy and live birth rates in those who performed a letrozole FET vs a medicated FET. Miscarriage rates were lowest for natural FETs.
They also split up the groups into women who were ovulatory or anovulatory/PCOS. For ovulatory women, ongoing pregnancies and live birth rates were higher in those who had a letrozole FET vs a medicated FET. There were no differences between the FET protocols in anovulatory/PCOS women.
A limitation of this study was that there was selection bias, meaning that the doctors were more likely to assign certain patients to one type of an FET over another, based on their diagnosis.
Anovulatory patients, or those with PCOS, were more likely to be assigned to medicated FETs or letrozole FETs. This is why there were differences in the baseline patient and cycle characteristics as indicated above. However all of these aspects were controlled for in their statistical adjustments and significant results were still found.
Because anovulatory/PCOS patients saw no benefit with medicated FETs over letrozole FETs, the authors suggest that letrozole FETs may be a better option for these patients.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols
 Survey examines the use and attitude of natural cycle FETs in US clinics
Survey examines the use and attitude of natural cycle FETs in US clinics
 Identifying the optimal timing for embryo transfer in modified natural and natural FETs
Identifying the optimal timing for embryo transfer in modified natural and natural FETs
 Pregnancy outcomes and complications with medicated, natural and mild stimulated FETs
Pregnancy outcomes and complications with medicated, natural and mild stimulated FETs
 Worsened perinatal and obstetric outcomes for medicated FETs vs modified natural FETs
Worsened perinatal and obstetric outcomes for medicated FETs vs modified natural FETs
 Study finds more flexible triggering timing for modified natural cycle FETs
Study finds more flexible triggering timing for modified natural cycle FETs
 Same live birth rate, fewer complications with natural frozen embryo transfer
Same live birth rate, fewer complications with natural frozen embryo transfer
 Optimizing natural FET protocols: key results from a meta-analysis
Optimizing natural FET protocols: key results from a meta-analysis