Researchers in a 2022 study compared modified natural and medicated FETs and found that medicated FETs generally had worsened perinatal and obstetric outcomes, with no differences in neonatal outcomes.
There are a number of options for endometrial preparation for a frozen embryo transfer (FET), including a medicated or a natural FET. Check out my post on the different FET protocols to learn more about them.
Takeshima et al. (2022), in their retrospective study, compared perinatal, obstetric and neonatal outcomes after modified natural FETs or medicated FETs at a single center in Japan between 2008 and 2017.
There were a total of three groups in this study: women who had a medicated FET (n=5,318), women who had a modified natural FET and transferred 4.5 days after ovulation (n=29,705) or 5.0 days after ovulation (n=31,995).
For simplicity I’ll just be including the ovulation 4.5 group in this summary as the modified FET group. There were no statistically significant differences in outcomes between the 4.5 and 5.0 group*, and all their statistical analysis was done using the 4.5 group as a reference.
*With the exception of clinical pregnancy rates that were only off by 1% or so.
Key information:
- Women were minimally stimulated with clomid when they had their retrieval. It was not stated how long they waited until FET after retrieval.
- All frozen transfers involved single blastocysts (day 5).
- Modified natural FETs used buserelin as a trigger (not hCG).
- The ovulation 4.5 group transferred embryos 6 days after trigger.
- Medicated FETs used dyhydrogesterone and intravaginal progesterone and embryos were transferred 4 days after initiation.
- Only singleton pregnancies were included.
- To report outcomes, women were asked to fill out a questionnaire. If they didn’t respond, the researchers conducted a follow-up.
In terms of baselines characteristics, there were a number of differences between the study groups (confounders). Most of the differences were small but significant because of the large sample size. In their analysis, they statistically adjusted for age, BMI, smoking status, previous delivery, cause of infertility, embryo culture time and blastocyst morphology.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Pregnancy rates higher in modified natural FETs compared to medicated FETs
Clinical pregnancy rates were increased with modified natural FETs compared to medicated FETs (51.2% vs 47.0%, p<0.05).

Perinatal outcomes for modified natural FETs vs medicated FETs
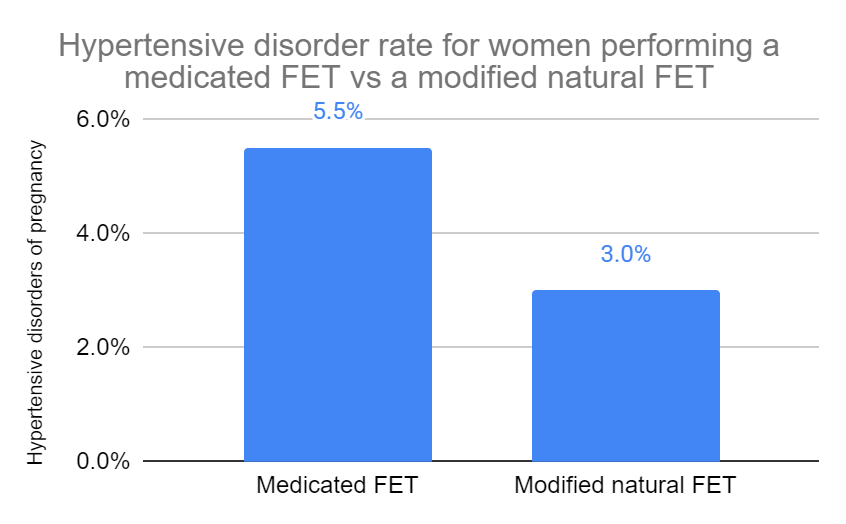
Hypertensive disorders of pregnancy were higher with medicated FETs compared to modified natural FETs (5.5% vs 3.0%, adjusted odds ratio [95% CI]: 2.17 [1.67-2.81]). This means that after adjustment for confounders (age, BMI, etc.), medicated FET pregnancies were 2.17 times more likely to exhibit hypertensive disorders compared to modified natural FETs.
Placenta accreta was higher with medicated FETs compared to modified natural FETs (0.5% vs 0.2%, adjusted odds ratio [95% CI]: 3.85 [1.54-9.60]). This means that after adjustment for confounders (age, BMI, etc.), medicated FET pregnancies were 3.85 times more likely to exhibit placenta accreta compared to modified natural FETs.
There were no differences in:
- Gestational diabetes (3.5% vs 4.2%)
- HELLP (Hemolysis, Elevated Liver enzymes and Low Platelets) syndrome (0.2%)
- Preterm premature rupture of membranes (0.3% vs 0.4%)
- Low-lying placenta (0.8% vs 0.5%)
- Placenta previa (1.6%)
- Placental abruption (0.3%)
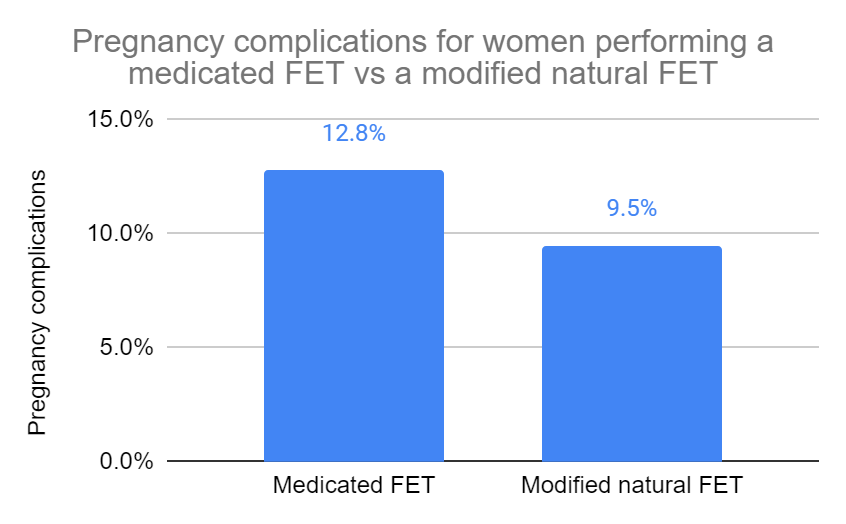
Overall pregnancy complications (including all of the above) during the perinatal period were higher for medicated FETs compared to modified natural FETs (12.8% vs 9.5%, adjusted odds ratio [95% CI]: 1.55 [1.30-1.84]). This means that after adjustment for confounders (age, BMI, etc.), medicated FET pregnancies were 1.55 times more likely to exhibit hypertensive disorders compared to modified natural FETs.
Perinatal outcomes for modified natural FETs vs medicated FETs
Cesarean delivery rates were higher for medicated FETs compared to modified natural FETs (43.4% vs 33.1%, adjusted odds ratio [95% CI]: 1.94 [1.71-2.19]). This means that after adjusting for confounders (age, BMI, etc.), medicated FET pregnancies were 1.94 times more likely to result in a cesarean delivery compared to modified natural FETs.

Preterm delivery rates (<37 weeks) were higher for medicated FETs compared to modified natural FETs (8.1% vs 5.5%, adjusted odds ratio [95% CI]: 1.54 [1.24-1.92]). This means that after adjusting for confounders (age, BMI, etc.), medicated FET pregnancies were 1.54 times more likely to result in a preterm delivery (<37 weeks) compared to modified natural FETs.
Low birthweight rates (<2500 g) were higher for medicated FETs compared to modified natural FETs (adjusted odds ratio [95% CI]: 1.43 [1.18-1.73]). This means that after adjusting for confounders (age, BMI, etc.), medicated FET pregnancies were 1.43 times more likely to result in a baby with a low birthweight (<2500 g) compared to modified natural FETs.
There were no differences in:
- Stillbirths (0.4% vs 0.2%)
- Small for gestational age (4.2% vs 4.9%)
- Large for gestational age (16.8% vs 16.6%)
- Infant death (0.1% vs 0.2%)
- Birth defects (2.5% vs 2.7%)
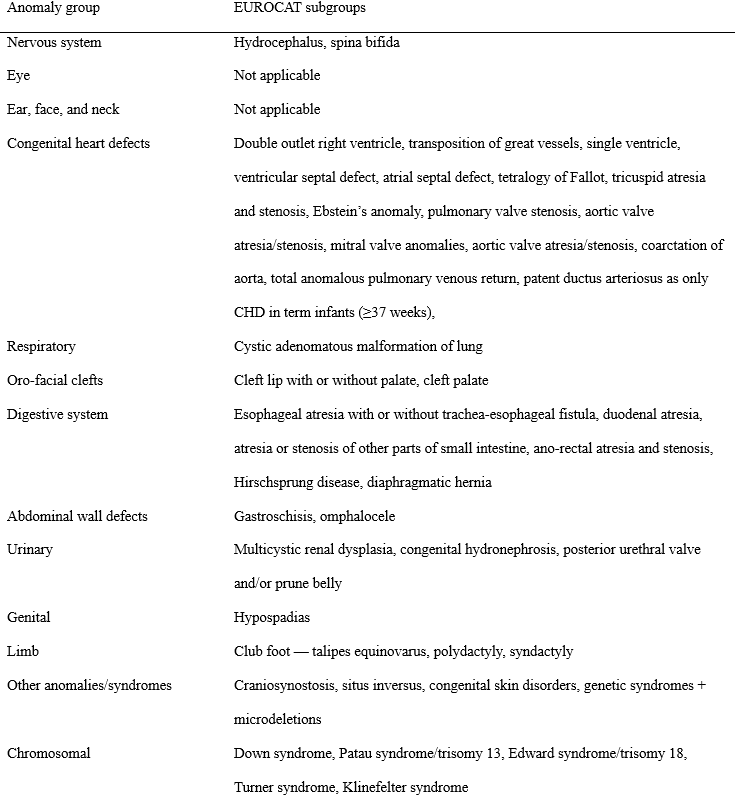
Congenital anomalies for modified natural FETs vs medicated FETs
There were no differences in:
- Nervous system congenital anomalies (0.2% vs 0.1%)
- Congenital heart defects (1.2% vs 1.5%)
- Respiratory congenital anomalies (0.0% vs 0%)
- Orofacial clefts (0.1% vs 0.1%)
- Digestive system congenital anomalies (0.1% vs 0.1%)
- Abdominal defects (0.0% vs 0%)
- Urinary congenital anomalies (0.3% vs 0.2%)
- Genital congenital anomalies (0.0% vs 0.1%)
- Limb congenital anomalies (0.2% vs 0.4%)
- Chromosomal congenital anomalies (0.4% vs 0.1%)
Here’s a table showing what they were looking for in each of these categories:
Conclusions
This study found that women who performed a medicated FET vs a modified natural FET had:
- Reduced clinical pregnancy rates
- Increased risk of hypertensive disorders of pregnancy
- Increased risk of placenta accreta
- Increased risk of overall pregnancy complications
- Increased risk of cesarean delivery
- Increased risk of preterm delivery
- Increased risk of low birthweight
There were a number of perinatal and obstetric outcomes that showed no difference after a medicated vs modified natural FET. There were no differences in congenital anomalies seen between the groups.
Some of the strengths of this study include:
- Large sample size
- Consistent ovarian and endometrial preparation, transfer protocols, etc. (single center)
Some of the limitations of this study include:
- A modified natural FET was the default, and medicated FETs were chosen for women with severe ovulatory failure or ovarian or luteal insufficiency. Women with diminished ovarian reserve (DOR) may have been more likely to receive a medicated FET and this wasn’t statistically adjusted.
- Women were free to choose a natural or medicated FET and there may have been bias associated with this.
- Self-reported questionnaires were used to report outcomes and there could have been reporting errors.
- Buserelin was used to trigger modified natural FETs and not hCG.
As frozen-thawed transfers become the mainstream method of ART, the [medicated FET] method of endometrial preparation will become increasingly convenient given that it allows easy schedule adjustment. However, further follow-up is needed to investigate these risks and explore improved endometrial preparation methods.
Takeshima et al. (2022)
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Pregnancy outcomes and complications with medicated, natural and mild stimulated FETs
Pregnancy outcomes and complications with medicated, natural and mild stimulated FETs
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols
 Comparing pregnancy outcomes for letrozole, natural and medicated FETs
Comparing pregnancy outcomes for letrozole, natural and medicated FETs
 Identifying the optimal timing for embryo transfer in modified natural and natural FETs
Identifying the optimal timing for embryo transfer in modified natural and natural FETs
 Survey examines the use and attitude of natural cycle FETs in US clinics
Survey examines the use and attitude of natural cycle FETs in US clinics
 Study finds more flexible triggering timing for modified natural cycle FETs
Study finds more flexible triggering timing for modified natural cycle FETs
 Same live birth rate, fewer complications with natural frozen embryo transfer
Same live birth rate, fewer complications with natural frozen embryo transfer
 Optimizing natural FET protocols: key results from a meta-analysis
Optimizing natural FET protocols: key results from a meta-analysis