A 2026 randomized trial found that natural FETs had similar healthy live birth rates to medicated FETs, but were linked to lower risks of preeclampsia, pregnancy loss, and some other pregnancy complications.
During a frozen embryo transfers (FET), the uterus can be prepared in different ways so the lining is ready for implantation.
Two of the most common options are medicated FETs and natural FETs. Natural FETs follow the body’s own ovulation and hormone production, but they require closer monitoring and are more likely to be cancelled. In medicated FETs, these hormones are added as medications instead, which makes the cycle easier to schedule.
Some evidence shows that medicated FETs are linked to preeclampsia and other pregnancy complications. It’s also not clear if one approach is better than another in terms of live birth rates.
A large, multicenter randomized controlled trial by Wei et al. (2026) was designed to compare natural and medicated FET cycles, looking not only at live birth, but also at maternal safety during pregnancy.
For more background, check my post on comparing frozen embryo transfer protocols.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: Multicenter randomized controlled trial conducted across 24 academic fertility centers in China between 2022 and 2023.
- Participants: 4,376 ovulatory women aged 20–40 planning a frozen single blastocyst transfer. Patients with 2 or more failed transfers, history of a thin endometrium (<7 mm), ovulatory dysfunction were excluded. Participants were randomized 1:1 to:
- 2185 natural FET cycles (true natural: 1335, modified natural: 540) and 2191 medicated FET cycles (intention-to-treat group).
- After protocol deviations, there were 1844 patients in the natural FET group and 1875 patients in the medicated FET group (per-protocol group).
- Embryos: Mostly single blastocyst transfers (>96%); both day 5 and day 6 blastocysts included with quality 4BC or higher. PGT-A was done in about 8% of cycles.
- Primary outcomes: Healthy live birth (born 37 weeks or later, with normal birthweight and no congenital anomalies) and pre-eclampsia or eclampsia.
- Trial registration: ChiCTR2200057990.
Natural FETs lowered preeclampsia risk without changing healthy live birth rates
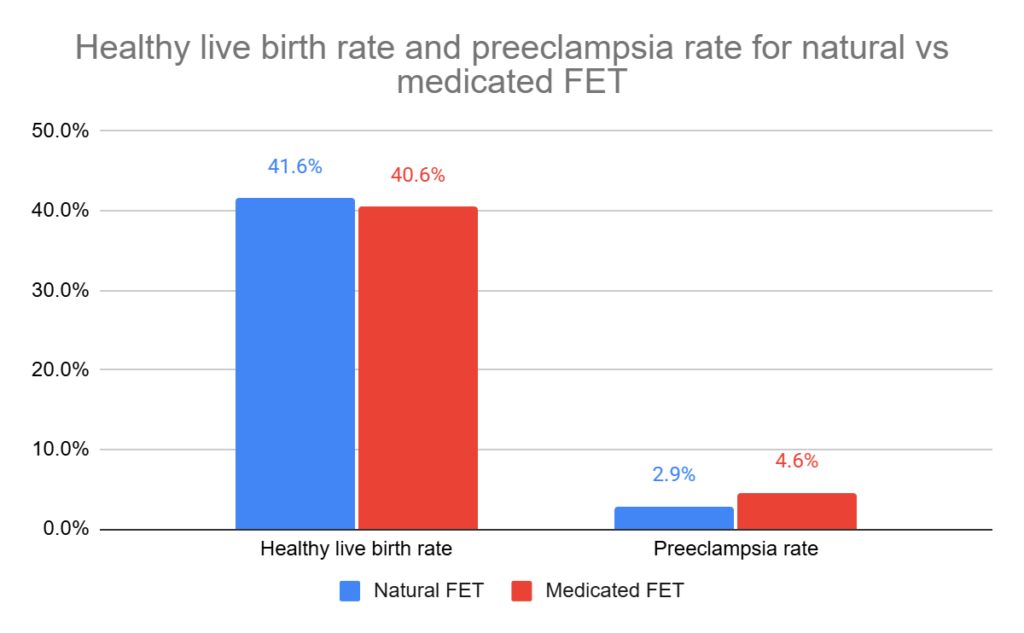
This study examined healthy live birth rates and preeclampsia risk in patients having a natural or medicated FET.
- No difference in healthy live birth rate for natural FET vs medicated FET (41.6% vs 40.6%, relative ratio [95% CI]: 1.03 [0.96-1.10], p= 0.49).
- Lower risk of preeclampsia with natural FET vs medicated FET (2.9% vs 4.6%, relative ratio [95% CI]: 0.63 [0.43-0.94], p= 0.02). This represents a ~40% decrease in the risk of preeclampsia with a natural FET.
These results were from the intention-to-treat analysis, and the findings were similar in the per-protocol analysis. There were no differences between true natural and modified natural FETs.
Overall, this shows that natural FETs achieved similar healthy live birth rates to medicated FETs, while reducing the risk of preeclampsia during pregnancy.
Natural FETs were linked to a lower risk of pregnancy loss
The researchers also examined live birth, clinical pregnancy, and pregnancy loss outcomes in patients having a natural vs medicated FET.
- No difference in live birth rate for natural vs medicated FET (51.1% vs 50.1%).
- No difference in clinical pregnancy rate for natural vs medicated FET (59.6% vs 60.5%).
- Lower risk of pregnancy loss with natural FET vs medicated FET (13.9% vs 16.9%, relative ratio [95% CI]: 0.82 [0.69-0.99], p= 0.03).
- Higher risk of cycle cancellation with natural FET vs medicated FET (16.2% vs 11.5%, p< 0.001). This was mainly due to no follicle development or arrested follicle development.
- No differences between true natural and modified natural FETs.
Overall, this suggests that while natural and medicated FETs led to similar chances of becoming pregnant and delivering a baby, natural FETs were associated with a lower risk of pregnancy loss after a clinical pregnancy.
Fewer pregnancy-related complications with natural FETs
The study also compared maternal and newborn complications after FET.
Natural FETs were associated with lower rates of several pregnancy-related complications, including hypertensive disorders of pregnancy (driven mainly by lower late-onset pre-eclampsia), placenta accreta spectrum, postpartum hemorrhage, and caesarean delivery.
Most other outcomes were similar between natural and medicated FETs, including ectopic pregnancy, gestational diabetes, early-onset pre-eclampsia, placenta previa, placental abruption, preterm birth, stillbirth, and a wide range of newborn outcomes such as birth weight, NICU admission, and congenital anomalies.
Conclusions
This study found that natural and medicated FETs had similar healthy live birth rates in patients who ovulate regularly. The main difference was pregnancy safety. Natural FETs were linked to a ~40% lower risk of preeclampsia, especially late-onset preeclampsia, although the overall risk was low.
Natural FETs were also linked to a lower risk of pregnancy loss after a clinical pregnancy, as well as lower rates of some other complications, including placenta accreta spectrum, postpartum hemorrhage, and caesarean delivery. Most other pregnancy and newborn outcomes were similar between the two approaches. Cycle cancellations were higher with natural FETs.
These differences may be because natural cycles form a corpus luteum after ovulation, which produces hormones that support blood flow and placental development. These hormones are given as medications in medicated FETs, which might not fully mimic the hormone environment in a natural cycle.
Other studies generally agree that natural FETs are linked to fewer pregnancy complications, but findings are mixed on whether they improve success rates.
Overall, this study suggests that natural FETs can offer similar chances of success with fewer pregnancy complications. The authors recommend using natural FETs when possible, especially for patients at higher risk of blood pressure problems, like older patients or those with obesity. Because this study was done in China, they note that the benefit could be even greater in countries like the US, where these risks are more common.
Limitations include a fairly high rate of protocol deviations (~15%), no direct measurement of corpus luteum hormones, differences in luteal support between clinics, limited ability to assess rare pregnancy and newborn complications, and results that may not apply to patients with irregular ovulation, thin endometrium, or repeated implantation failure.
Want to read more about natural FETs?

Researchers in a 2023 study found decreased adverse pregnancy and neonatal outcomes in those who performed a natural vs medicated FET, including abnormal birth weights, preeclampsia, preterm births, and more. Read more.

A 2025 randomized controlled trial found that natural cycle FETs led to higher live birth rates and fewer miscarriages than medicated FETs in ovulatory women with a good prognosis. Read more.
A 2026 study found that switching frozen embryo transfer protocols after a failed transfer did not improve live birth compared with repeating the same protocol, including in PGT-A cycles, with some small and uncertain differences seen in specific natural FET types. Read more.
Researchers in a 2022 study compared timing of euploid transfers and found that 160 h was optimal for modified natural FETs, while they found no optimal time for natural FETs. Read more.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.