Researchers in a 2022 study found no difference in live birth rates in those that transferred embryos by standard timing or timing established by the ERA.
The endometrial receptivity array (ERA, see here for more information) is a technique commonly used to identify the optimal time for embryo transfer.
Doyle et al. (2022) conducted a randomized controlled trial to compare euploid embryo transfers by standard timing (123 ± 3 hours) or timing determined by the ERA (Igenomix). To control for the biopsy procedure, all participants had an ERA biopsy performed. This was a multicenter study that included 767 participants across the US between 2018 and 2020.
Key points:
- Women were 30-40 years old
- Women with recurrent implantation failure (>2 transfers that failed) were excluded
- Women with recurrent pregnancy loss (≥2 clinical pregnancy losses without a live birth) were excluded
- Blastocysts at least BB in quality were used for PGT-A
Baseline characteristics were similar between the groups for age, mean BMI, prior live birth, prior failed transfer, endometrial thickness and day the embryo was frozen. Results of the ERA were similar between the standard and ERA-guided groups (approximately the same rates of receptive, nonreceptive, pre-receptive, early receptive, late receptive and post receptive).
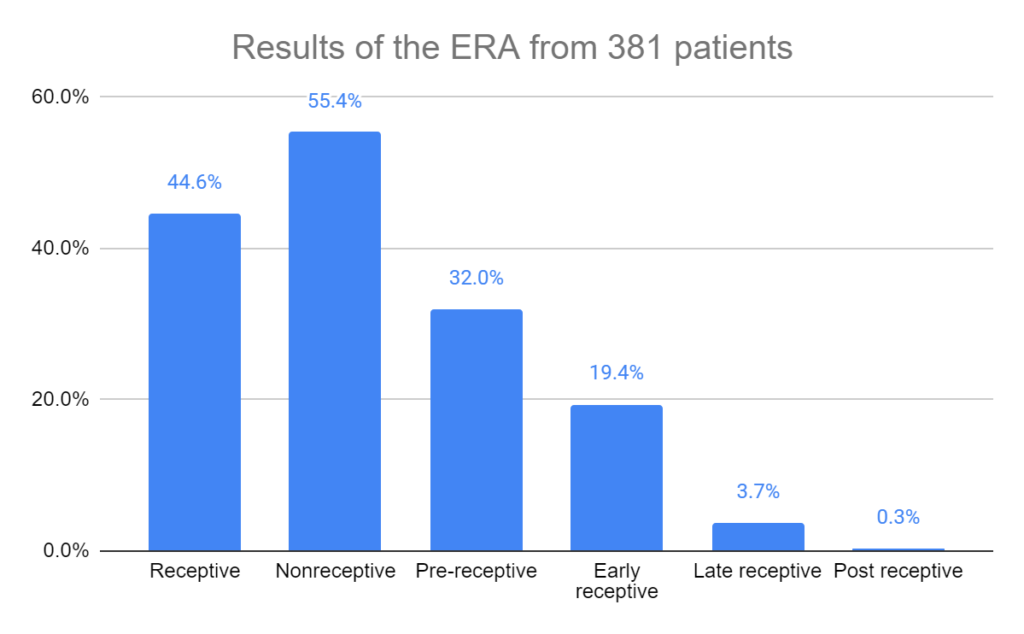
The results presented here will include only the intention-to-treat analysis, which includes people who were registered in the trial but dropped out for whatever reason. In this study there were 767 participants that were split between the standard (n=381) and ERA-guided (n=386) groups before embryo transfer. A total of 12 participants dropped out between this stage and after transfer (6 from each group), which is what was used for the per-protocol analysis. In all cases the intention-to-treat and per-protocol analyses were comparable.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
No differences in live birth or clinical pregnancy rates after the ERA
There were no statistically significant differences in live births between ERA-guided and standard transfer groups (58.5% vs 61.9%, difference [95% CI]: -3.4% [-10.3% to 3.5%]). There was also no difference in clinical pregnancies (68.8% vs 72.8%, difference [95% CI]: -4.0% [-10.4% to 2.4%]).

No difference in total pregnancy losses with the ERA
There were no statistically significant differences between ERA-guided and standard transfer groups in terms of biochemical losses (9.9% vs 8.1%, difference [95% CI]: -1.8% [-2.8% to 6.4%]), clinical pregnancy losses (13.7% vs 14.6%, difference [95% CI]: 0.9% [-6.8% to 5.0%]) and total losses (22.1% vs 21.5%, difference [95% CI]: -0.6% [-6.0% to 7.2%]).
Possibly no difference with ERA for timing adjustments ≥12 hours
In an analysis that took place after the trial was completed (post-hoc), they examined ERA nonreceptive patients that required adjustment of progesterone ≥12 hours. The authors state that this analysis was underpowered and should be considered for future research.
In terms of ERA-guided and standard timing, there were no differences in live birth rates (54.5% vs 62.5%, difference [95% CI]: -8.0% [-17.3% to 1.5%]) and clinical pregnancy rates (65.4% vs 74.5%, difference [95% CI]: -9.1% [-17.8% to -0.4%], p=0.06).
Possible worsened biochemical losses, pregnancy rates with ERA for timing adjustments ≥24 hours
In an analysis that took place after the trial was completed (post-hoc), they examined ERA nonreceptive patients that required adjustment of progesterone ≥24 hours. The authors state that this analysis was underpowered and should be considered for future research.
For ERA-guided vs standard timing, there were no differences in live birth rates (54.5% vs 63.3%, difference [95% CI]: -8.8% [-21.1% to 3.5%]) but there was a decrease in clinical pregnancy rates (61.8% vs 78.3%, difference [95% CI]: -16.5% [-27.8% to -5.2%], p=0.01).

There was an increase in biochemical pregnancy losses with the ERA (15.2% vs 4.0%, difference [95% CI]: 11.2% [2.9% to 19.5%], p=0.02).
Conclusions
This study found no differences when using ERA-guided timing or standard timing for euploid transfers, in terms of pregnancy or live birth rates, biochemical losses, clinical pregnancy losses and total losses.
An analysis performed after the RCT (post-hoc) found a decrease in clinical pregnancy rates when the ERA required ≥24 hours of adjustment, compared to the standard timing group. However the authors state that this analysis was underpowered (so this result may not be reliable).
A limitation of this study is that RIF and RPL patients were not included, who are claimed to be the group that would benefit most from the ERA.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Meta-analysis finds no difference in pregnancy outcomes when using the ERA
Meta-analysis finds no difference in pregnancy outcomes when using the ERA
 IVF pregnancy outcomes after intrauterine PRP: a 2022 clinical trial
IVF pregnancy outcomes after intrauterine PRP: a 2022 clinical trial
 ERA-timed euploid transfers shows no benefit over standard timing
ERA-timed euploid transfers shows no benefit over standard timing
 Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
 Intrauterine hCG for IVF patients improves pregnancy rates
Intrauterine hCG for IVF patients improves pregnancy rates
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 Silent insulin resistance is common, linked to lower IVF success rates
Silent insulin resistance is common, linked to lower IVF success rates