A 2025 study found that nearly one in three IVF patients without PCOS or diabetes had insulin resistance, which was linked to lower success rates, but taking metformin before embryo transfer seemed to help.
Glucose is the body’s main energy source, and insulin is the hormone that helps move it into cells. After meals, insulin signals cells to absorb glucose from the blood. When this process doesn’t work well, it’s called insulin resistance.
Insulin resistance is most often discussed in the context of PCOS, where it affects 35–80% of patients, but many people without PCOS also have it, often without knowing. It can occur in people with normal weight, and common screening tools may miss it.
There’s growing evidence that insulin resistance is linked to a higher risk of pregnancy loss. One reason may be that insulin helps the endometrium take in glucose and build up energy stores (in the form of glycogen) needed for implantation.
Metformin is a medication that improves insulin sensitivity. In PCOS patients, metformin is sometimes used during IVF to reduce OHSS risk and may also improve pregnancy outcomes, though results have been mixed. But its role in non-PCOS patients with IR hasn’t been well studied.
A new study by Albert et al. (2025) looked at IVF outcomes in non-PCOS women with and without insulin resistance (measured with an oral glucose tolerance test), and whether metformin treatment before embryo transfer might improve success. Patients did not have PCOS, were not obese, and did not have diabetes. Donor eggs were used to control for the effect of egg quality.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- This was a retrospective cohort study using data from 17 IVF clinics in Spain between 2015 and 2023.
- Women were between 18-45, not obese (BMI 30 or lower), without PCOS or diabetes.
- All patients used donor eggs and their first embryo transfer results were reported.
- Insulin resistance was measured with an oral glucose tolerance test (patients with elevated plasma insulin of >10, >100, >60 mcU/ml at 0, 60 and 120 min following an overnight fast and 75 g oral glucose were considered insulin resistant)
- The most common metformin regimen was 850 mg/day that increased to 1700 mg/day if tolerated, started at least 1 month before transfer and maintained until the 12th week of pregnancy.
In terms of sample size, there were a total of 1033 patients: 315 with insulin resistance and 718 without. Of the 315 women with insulin resistance, 117 were treated with metformin and 198 weren’t.
In terms of baselines characteristics, there were some differences that were statistically adjusted (BMI, adenomyosis status, number of embryos transferred, day of embryos). The average age was about 40 for both groups and the average BMI was 22-23.
Nearly 1/3 of women showed insulin resistance
Even though none had PCOS or diabetes, an oral glucose tolerance test showed that 30.5% of the women had insulin resistance. In other words, nearly one in three had undiagnosed insulin resistance.
Women with insulin resistance had a higher BMI (compared to women who weren’t insulin resistant) and were more likely to have adenomyosis (13.1% vs 5.4%, p< 0.001).
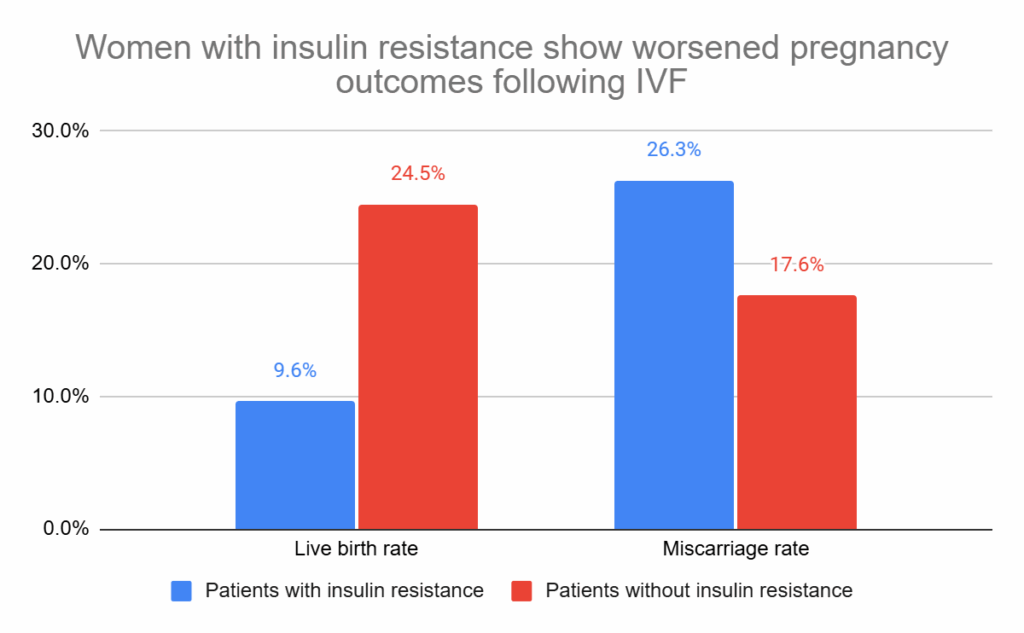
Women with insulin resistance have reduced live birth, higher miscarriage rates
Compared to women without insulin resistance, women with insulin resistance had higher miscarriage rates (26.3% vs 17.6%) and lower live birth rates (9.6% vs 24.5%). After statistical adjustment, these were both statistically significant (adjusted relative risk [95% CI]: 1.44 [1.09-1.92], p= 0.013; adjusted relative risk [95% CI]: 0.42 [0.27-0.66], p< 0.001).
Metformin is associated with improved outcomes in insulin resistant women
Insulin-resistant women that were treated with metformin had better outcomes than those untreated: lower miscarriage (13.7% vs 26.3%), and higher live birth rates (40.2% vs 9.6%). After statistical adjustment, these were both statistically significant (adjusted relative risk [95% CI]: 0.481 [0.288-0.804], p= 0.005; adjusted relative risk [95% CI]: 4.069 [2.445-6.774], p< 0.001).
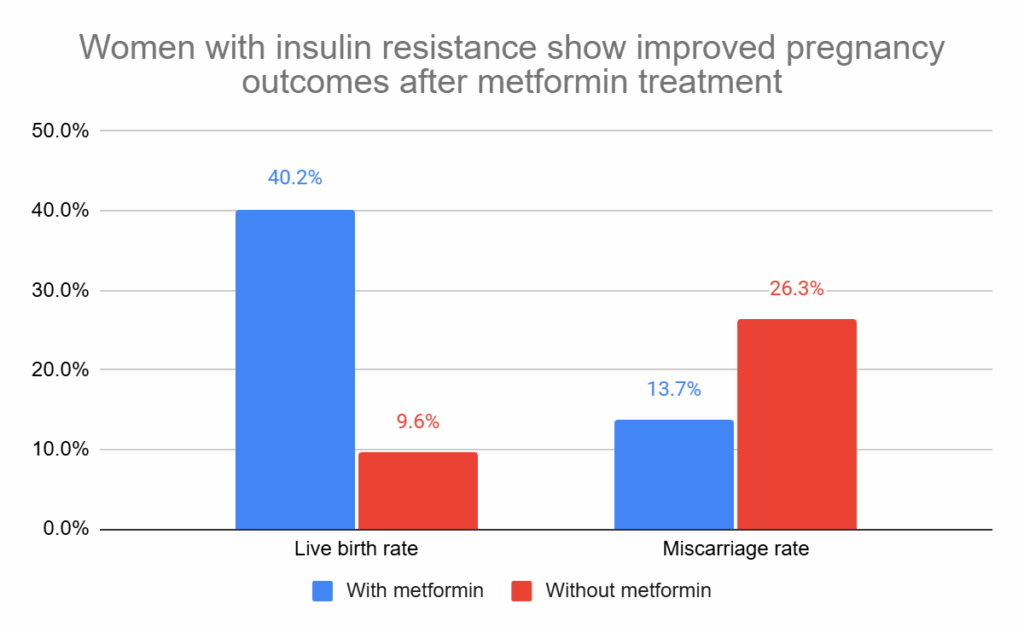
This is pretty impressive, and shows that metformin could increase the live birth rate by about 4 times in patients with insulin resistance.
Conclusions
This study showed that nearly 1/3 of women without PCOS or diabetes undergoing IVF had insulin resistance.
These insulin resistant women had lower live birth rates and higher miscarriage rates, which were both improved after metformin treatment.
Importantly, these women all used donor eggs, so the reduction in live birth rate is likely the related to the uterine environment.
Biologically, this may relate to how insulin regulates glucose uptake and the buildup of energy stores (glycogen) in the endometrium, which is critical for implantation. Metformin may help improve this function in women with insulin resistance.
Previous studies have shown that insulin resistance worsens IVF outcomes in women with PCOS, but evidence in non-PCOS women is limited and mixed (referenced below).
Many women can have insulin resistance even without a diagnosis of prediabetes or diabetes, often because of factors like genetics, aging, excess weight, diet, or lack of exercise (source: Nebraska Med).
This study suggests that screening for insulin resistance in non-PCOS patients could be worthwhile. For those who are insulin-resistant, metformin treatment may help improve the uterine environment, though further randomized trials are needed. Lifestyle modifications such as diet and exercise may also help improve insulin sensitivity and support better IVF outcomes.
Limitations include the retrospective design, possible unmeasured confounders (eg. diet, stress, other medications), variation in metformin dosage/duration, and lack of data on endometrial insulin sensitivity. Also, the study did not include a metformin-treated group in women without insulin resistance, so the findings apply only to insulin resistant patients.
Related studies
These additional studies were referenced by the authors of the paper and haven’t been covered on Remembryo. They may be helpful if you’re exploring this topic further. This section is available for paid subscribers.

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Endometrial thickness and pregnancy outcomes after 96,000 embryo transfers
Endometrial thickness and pregnancy outcomes after 96,000 embryo transfers
 Meta-analysis finds no difference in pregnancy outcomes when using the ERA
Meta-analysis finds no difference in pregnancy outcomes when using the ERA
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer
 Meta-analysis examines impact of small fibroids on pregnancy outcomes
Meta-analysis examines impact of small fibroids on pregnancy outcomes
 Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
 Intrauterine hCG for IVF patients improves pregnancy rates
Intrauterine hCG for IVF patients improves pregnancy rates
 Early beta-hCG detection after transfer distinguishes normal from delayed implantation
Early beta-hCG detection after transfer distinguishes normal from delayed implantation