Not sure what your embryo grade means—or if it affects your chances of success? This guide walks you through everything from day 3 and day 5 grading systems to what each number and letter combo (like 3BB or 5AA) actually means. You’ll also find success rate research, embryo photos, and insights from a former embryologist to help make sense of your report.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
The stages of embryo development
Here we’ll look at how a fertilized egg after IVF changes from a single cell into a blastocyst over the course of about 5 days. This is crucial information to understanding embryo grading! There are different stages as the embryo develops, including the cleavage stage, morula stage and the blastocyst stage.

Fertilization and the pronuclear stage (day 0)
This isn’t really a stage for an embryo’s development, but is when the egg is fertilized, or combined with sperm, as a part of IVF. The day eggs are fertilized is considered day 0. If eggs are fertilized right after the egg retrieval, then the day of the egg retrieval will be day 0. Alternatively, frozen eggs can be thawed and fertilized, and the day the eggs are thawed will be day 0.
Eggs can be fertilized by conventional IVF or by intracytoplasmic sperm injection (ICSI). In conventional IVF, sperm are mixed with the eggs and left to fertilize. During ICSI, a single sperm is injected into an egg to fertilize.
Fertilization is where the gametes (sex cells, like the egg and sperm cell) come together to form the embryo. You can actually tell fertilization is occurring because you can see the nucleus of the egg and sperm cell (called the pronuclei, as plural). The result is a fertilized egg, sometimes called a zygote.

Cleavage stage (day 1 – day 3)
Over the next few hours the zygote has its first cell division to make 2 cells (once it becomes 2 or more cells, the zygote is called an embryo), and then another after about 24 hours to 4 cells, then to 8, etc. These are “cleavage stage” embryos because the cells cleave, or split, to form a new cell. The number of cells is important for cleavage stage embryo grading, as we’ll see.
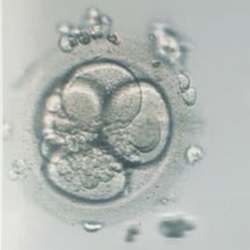
Here’s an example of a cleavage stage embryo with around 8 cells:

Morula stage (day 4)
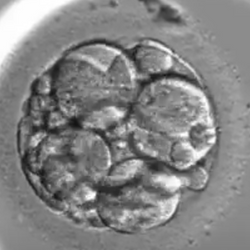
Usually around day 4 the cells undergo compaction to form a “morula.” I equate this to a kind of cocoon where the cells of the embryo start to change, or differentiate, into the cells of the blastocyst, which is a very different structure compared to the cleavage stage embryo.
The word “morula” comes from the Latin word “morus” which means a mulberry, or blackberry, which is kind of what it looks like!
The individual cells that you were able to make out during the cleavage stage are harder to see during the morula stage because they start to merge with each other. How compacted a morula becomes through this merging process is important for morula embryo grading.
Here’s an example of a morula below:
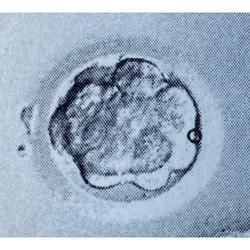
Blastocyst stage (day 5+)
Usually around day 5 or so, the blastocyst forms.
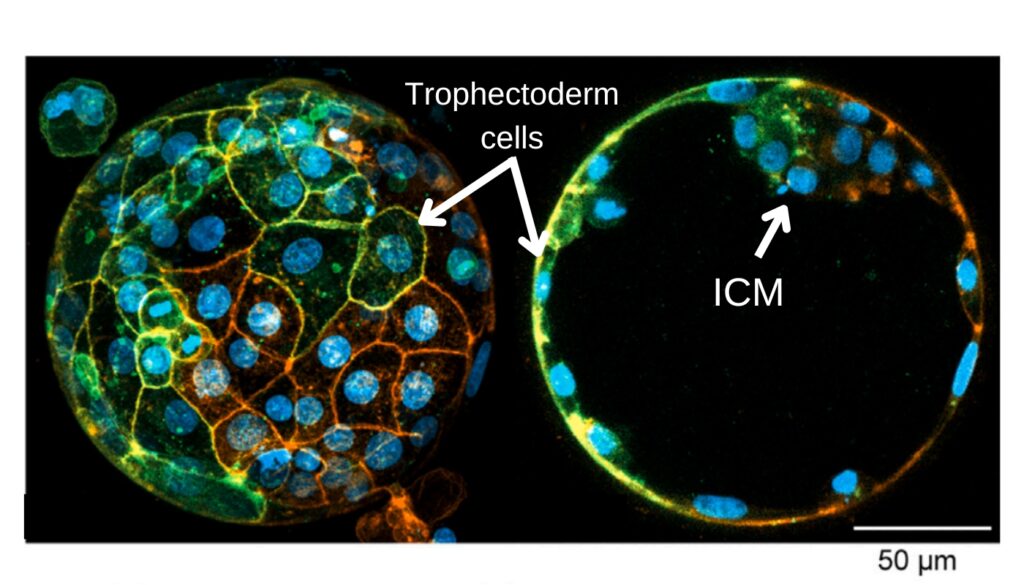
There are two main types of cells in a blastocyst: the inner cell mass (ICM) and the trophectoderm. The ICM actually becomes the fetus, while the trophectoderm becomes the placenta! These two cell types are important when it comes to blastocyst embryo grading.

Surrounding the blastocyst is the zona pellucida, or zona for short, which is like a shell that was originally present in the egg and carried on. If you look back at the previous pictures, you’ll see the zona is there also.
A blastocyst is kind of like a water balloon. The skin of the balloon is made up of the trophectoderm cells that surround a cavity called the “blastocoel,” which is filled with water. Inside this water-filled cavity is the ICM stuck to the inside at some position.

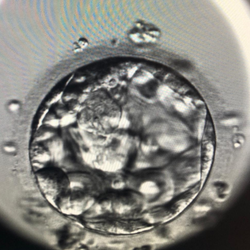
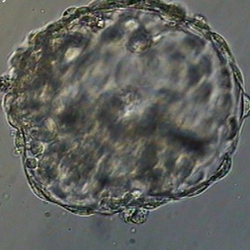
Here’s another image of a blastocyst, that’s been stained so you can see the individual trophectoderm cells. Each blue circle is the nucleus of a cell. On the left you can see the outside of the blastocyst, surrounded by the trophectoderm cells, and on the right you can see a cross-section of the blastocyst that shows the blastocoel cavity. On the right, you can see the individual trophectoderm cells surrounding this cavity, with the ICM toward the top.
Depending on how developed the blastocyst is, it can be called an “early blastocyst”, an “expanded blastocyst” or a “hatching blastocyst.” Eventually the embryo gets so large that it hatches or breaks free from its zona and the sticky trophectoderm cells stick to the lining of the uterus to begin implantation and a pregnancy!
What is embryo grading?
Embryo grading is where an embryologist evaluates an embryo under a microscope and looks for key features. These features depend on what stage of development the embryo is in.
For cleavage stage embryos, or day 2 or day 3 embryos, these features are typically:
- The number of cells
- The amount of fragmentation
- How similar in size each cell is
For morulas, these features are typically:
- How compacted the morula is
For blastocysts, these features are typically:
- How big the blastocyst is
- The quality of the ICM
- The quality of the trophectoderm
In addition, the number of days it took the embryo to become a specific stage is considered. Sometimes embryos grow faster, and sometimes they grow slower. While many embryos become blastocysts on day 5, sometimes it takes longer (day 6 or day 7). The day of an embryo isn’t really part of the grade, but it’s considered as research has shown that how fast an embryo grows relates to its chance of implanting.
Why are embryos graded?
Embryos are graded to rank them for transfer. Different research has shown that embryos with better grades tend to have a higher chance of implanting and leading to a pregnancy.
So for example, if you have 2 embryos and one has a “good” grade and the other has a “poor” grade, the embryo with the good grade will be transferred first. This is because it’s more likely to lead to a pregnancy than the poorly graded embryo.
This doesn’t mean that a low quality embryo won’t go on to form a pregnancy. There’s a lot of research that has shown that embryos across all grades are able to lead to healthy births. But these embryos are considered after high quality embryos, because they’re less likely to work and doctors hope to get you pregnant as fast as possible!
We’ll get into all the statistics and the studies below, so stay tuned!
Cleavage stage embryo grading (day 2 or day 3 embryo grading)
Because of inconsistencies in grading cleavage stage embryos, in 2007 the Society for Assisted Reproductive Technology (SART) began requesting its US clinic members to report data in a specific way (Racowsky et al. 2011). This is based on:
- The number of cells in the embryo
- The amount of fragmentation (given as a percentage)
- How similar in size each cell is (symmetry)
This information can be gathered by examining the embryos under the microscope to give a grade which can be used as a ranking order for embryo transfer.
Most cleavage stage transfers these days are day 3 transfers, with fewer performing day 2 transfers. This post will mostly be with day 3 embryos in mind, but day 2 will be included where I can!
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Number of cells
The number of cells in a cleavage stage embryo has to do with how fast it divides. Embryos that have 8 cells on day 3 are dividing faster than embryos with 6 cells on day 3.
Often you’ll hear about an ideal number of cells, which is often stated to be 4 cells on day 2 and 8 cells on day 3. This is good as a general guide, but newer research is showing that embryos with more than 8 cells have comparable success rates to 8-cell embryos.
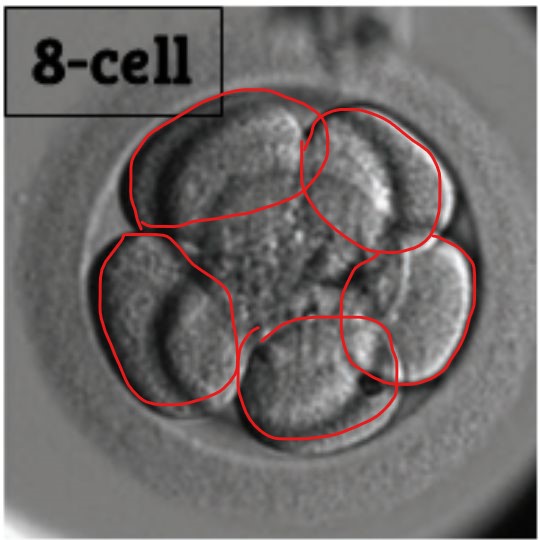
Here’s an example of what a 4 cell and 8 cell cleavage stage embryo looks like.

It’s pretty easy to see that the 4 cell embryo has 4 cells because they’re all immediately obvious from this particular picture. The 8 cell is a bit more challenging, because there are cells on top and below the plane of focus (where the microscope is focused). In fact, there are 5 cells that are in focus, with one cell on top and two below.
Here’s the 5 that are in focus:
Here are the two below the plane of focus:
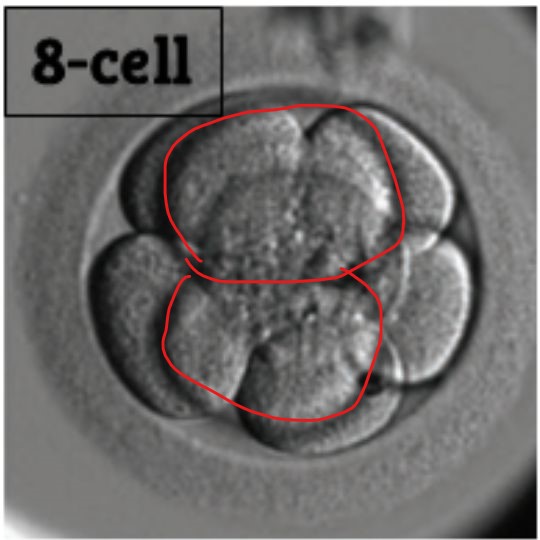
And here’s the one that’s above the plane of focus:
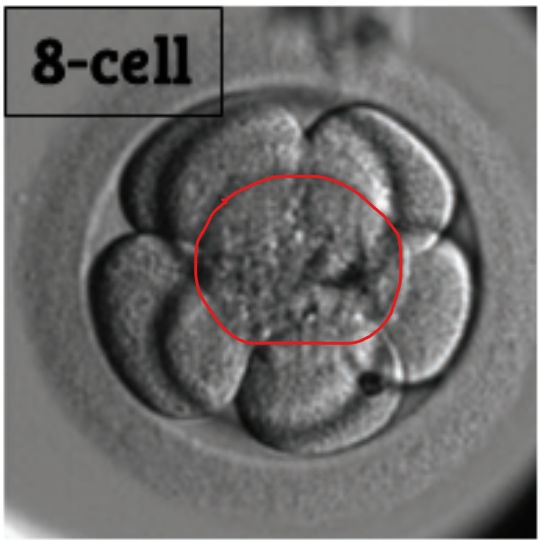
Here’s the original image blown up a bit, see if you can now see the 8 cells!

Fragmentation
Occasionally, as the cells of the embryo are dividing, there’s some tiny pieces called fragments that pop out. Fragmentation is usually written as a percentage of the whole embryo. You can see some examples of fragmentation in embryo pictures below:

As you can tell, it gets pretty hard to tell where the actual cells are when there’s more fragmentation. As fragments are lost, the cell that fragmented gets smaller. Imagine taking a snowball and ripping pieces off of it – the snowball itself gets smaller as each piece is removed.
Racowsky et al. (2011) show that SART’s parameters (0%, <10%, 10-25%, >25% fragmentation) correlate well with live birth rates. In general, many cleavage stage embryos receive their grade based on the amount of fragmentation:
- Good: <10% fragmentation
- Fair: 10-25% fragmentation
- Poor: >25% fragmentation
Cell symmetry (cell size)
Ideally when a cell divides they should both be the same size. This is called symmetry when referring to cleavage stage embryo grading. When the egg cell is fertilized and divides from one cell into two, those two cells are about half the volume of the first cell.
There’s a lot of components inside each cell, and this needs to be distributed equally. Uneven division may result in uneven distribution of proteins and other factors that the cell needs to develop normally (Rienzi et al. 2005).
Cleavage stage embryos with uneven cell size have lower implantation and pregnancy rates (Hardarson et al. 2001).
Generally, embryos with a high degree of fragmentation also show signs of irregular symmetry, because as fragments are lost the cell itself gets smaller.

How day 3 embryo grades are reported
Clinics can have different ways of reporting grades. I’ll explain the way I learned when I was an embryologist.
It’s based on two numbers, for example a 1/4:
The first number (1 in this case) is the quality. This refers to the quality of the embryo, or grade. Usually it’s based on the fragmentation:
- 1 (poor quality): >25% fragmentation
- 2 (fair quality): 10-25% fragmentation
- 3 (good quality): 1-10% fragmentation
- 4 (good quality): 0% fragmentation
The second number (4 in this case) is the number of cells. So in a 1/4 there’s 4 cells.
At least at my old clinic, the first number could vary based on factors besides fragmentation. So if there’s a low number of cells on day 3, like 4 for example, we might take off points to reflect this. So even if there was no fragmentation, the embryo would still be 1/4 because having 4 cells on day 3 is low quality.
These were kind of house rules, and weren’t dictated by any studies that I know of. It was just a way to avoid embryologists from thawing the wrong embryo because a 4/4 (good quality 4 cell embryo) might be confusing to some newer people who might want to thaw and transfer that over a 2/6.
Other clinics may have other house rules when it comes to day 3 embryo grading!
Here’s a quick guide that puts it all together:

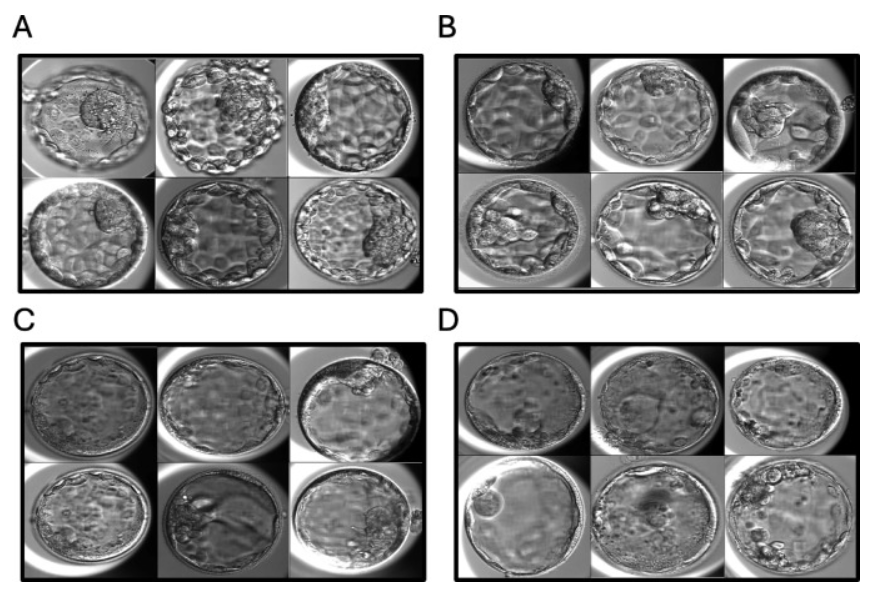
Day 3 embryo grades with pictures
Here are some pictures of day 3 embryos and their grades. This is from my Embryo Gallery where I post pictures of submitted embryo photos and their grades from my supporters. Check it out to see a lot more!




Day 3 embryo grades and success rates
Zhu et al. (2014) looked at Day 3 double embryo transfers (average age of 30). Good quality embryos had 7-8 cells and <10% fragmentation, while fair/poor had <5 cells and 30-50% fragmentation.
- Good quality embryos: 40%% live birth rate
- Fair/poor quality embryos: 11% live birth rate
- Miscarriages increased from 9% in the good group to 16% in the fair/poor group.
Awadalla et al. (2022) created models to predict live birth rates based on 223,377 embryo transfers in the US. You can see the graph below that shows the impact of cell number on predicted live birth after transferring a single fresh day 3 embryo.
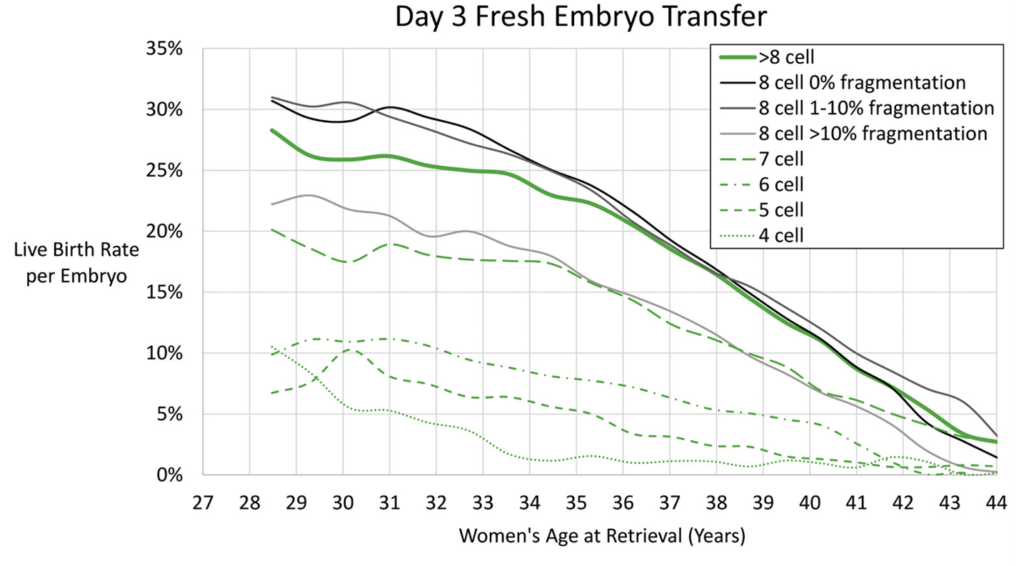
Notice how the chance of a live birth is predicted to decrease with age (discussed more below), and that day 3 embryos with fewer cells generally don’t do as well. Embryos with 7 or more cells on day 3 tend to have the best live birth rates based on this study, while embryos with 6 or fewer cells are predicted to do a bit worse.
This study also looked at frozen transfers, which were comparable. I have the full summary of this study on my post Predicting live birth rates, multiples based on 223,377 transfers.
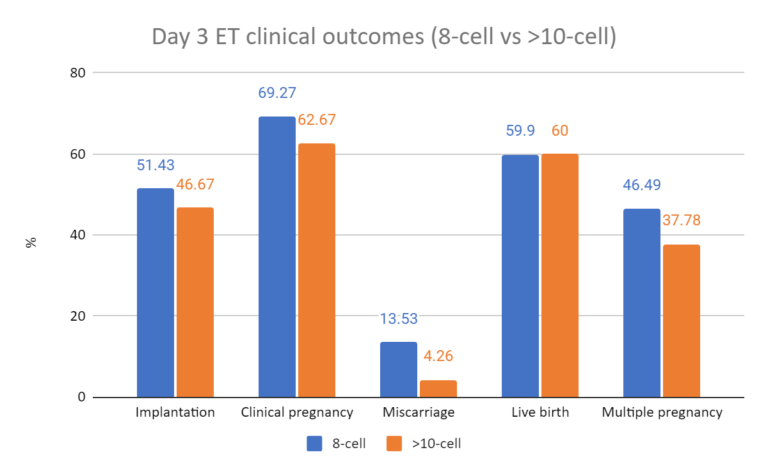
Zhao et al. (2019) took a closer look at embryos with more than 10 cells on day 3. These “fast growing” embryos are growing a bit faster because they have more than 8 cells on day 3.
They found that day 3 embryos with more than 10 cells had comparable implantation, pregnancy, live birth and multiple pregnancy rates compared to 8 cell embryos. However the miscarriage rate was lower when there was more than 10 cells.
If you want to check the full summary of this study, I have it on my post Fast growing day 3 embryos and their reproductive potential.
And let’s not forget about day 2 embryos!
Rhenman et al. (2015) examined day 2 single embryo transfers (average age 34):
- Cell number (day 2):
- Having 4 cells was ideal and resulted in ~30% live birth rate.
- 5 cells: ~18%
- ≥6 cells: 10%.
- 2-3 cells: ~3-8%.
- Fragmentation
- 0-10% fragmentation resulted in ~30% live birth rate.
- 10-25%: ~26%.
- 25-50%: ~23%.
- >50%: ~10%.
- Symmetry:
- All cells the same size resulted in ~30% live birth rate.
- <50% difference in cell sizes: ~23%.
💡 Want to see real success stories with day 3 embryos?
Check the IVF Success: Day 3 embryo collection from the Uterine Wall of Fame, which features a growing collection of IVF success stories submitted by people who have been through it themselves.
Poor quality embryos work – check your clinic’s policy on discarding them
You’ll notice from above that poor quality embryos may have reduced implantation rates and higher risks of miscarriage compared with higher graded embryos. Because of this, some clinics have minimum quality thresholds for transfer. It’s important to check with your clinic about their policies when planning a cycle.
There’s quite a bit of data I’ve compiled on these embryos, and you can check it out on my Grade C (poor quality) embryo success rates post, but here’s one of them:
- Zhu et al. (2014) compared pregnancy outcomes after transferring 2 good or 2 poor quality day 3 embryos and found a decrease in pregnancy rates (50.26% vs 16.15%), with an increase in miscarriages (13.28% vs 19.77%), but no differences in stillbirths, ectopic pregnancies, complications, birth weights and other birth outcomes.
💡 Want to see real success stories with lower-grade embryos?
Check the IVF Success: Poor quality embryo collection from the Uterine Wall of Fame, which features a growing collection of IVF success stories submitted by people who have been through it themselves.
Blastocyst embryo grading (Day 5 grading)
Blastocyst grading is done primarily using the Gardner system. This takes into account the size the blastocyst, also called the “expansion,” the quality of the inner cell mass (ICM) and the quality of the trophectoderm.
Below you can see a picture of a blastocyst with these structures indicated, as well as the zona (zona pellucida) which is the shell of the embryo.
For an embryo graded as “4AB:”
- The 4 is the expansion
- The A is the quality of the ICM
- The B is the quality of the trophectoderm
The expansion is the number portion and goes from 1-6, while the quality of the ICM and trophectoderm is indicated by a letter, where A is good, B is fair and C is poor.
To visualize a blastocyst, picture a blown up balloon with a golf ball inside stuck to one position. The rubber skin of the balloon is like the cells of the trophectoderm and the golf ball is the ICM. Instead of air, the embryo is filled with water and gets bigger, or expands, over time.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
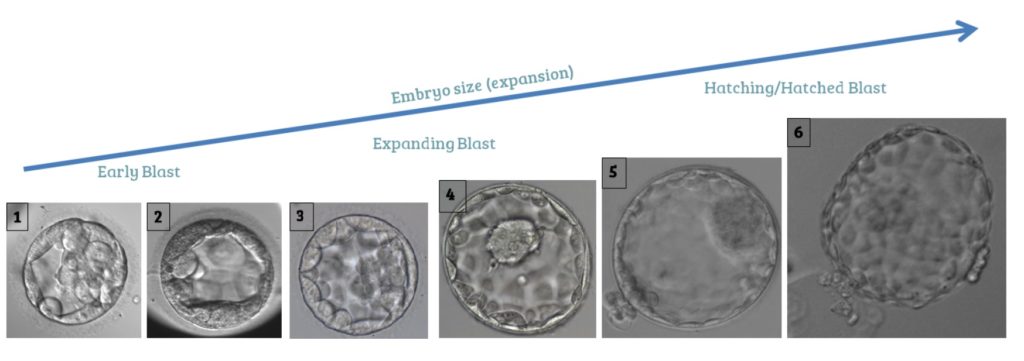
Expansion
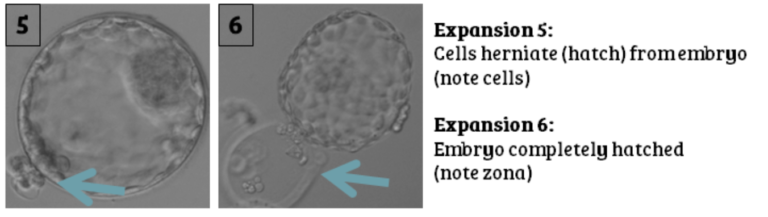
First let’s talk about the expansion (the size) of the embryo. There are 3 stages to an embryo’s expansion: early (1-2), expanding (3-4), hatching (5) and hatched (6).
What determines the embryo’s expansion? The blastocyst has a structure called a blastocoel which is the space inside the blastocyst that fills up with water. This cavity collects water and allows for the embryo to expand as it takes in more water.
During the early blastocyst stage the blastocoel is simply growing in size. The blastocoel is full at expansion stage 3 and when it reaches 4 the embryo itself is starting to grow larger. As it grows in size, the embryo stretches and thins out the zona. Eventually some cells start to hatch out from the zona (expansion 5) until ultimately the zona cracks open and the embryo is completely hatched (expansion 6).

It’s important to realize that as the embryo’s expansion number increases above 3, the embryo itself is getting bigger. Here’s another way to look at this:
Variability in expansion embryo grades by clinic or embryologist
There can be variability in grading the expansion depending on the clinic and the subjectivity of the embryologist.
Expansion 1 and 2 can be pretty variable because it’s sometimes not clear if the blastocoel is less than or more than 50%.
Expansions of 3 and 4 are also variable. The zona thinness is what determines if the embryo is a 4, and some clinics may only grade them as a 4 if the zona is very thin, while others may grade it a 4 if it’s only a bit thin. So what’s a 4 to one clinic may be a 3 to another.
Some clinics will also only call the embryo a 5 if there are many cells hatching out, while others have a lower threshold and might only require a single cell to be hatching out.
And then there’s biopsied embryos for PGT-A!
These embryos are assisted hatched, where the embryologist uses a laser to make a tiny hole in the zona. This usually happens on day 3, so by day 5 when the embryo is a blastocyst, the cells can easily hatch out. Because the cells can slip out easily, the zona doesn’t thin out as the embryo grows. Instead, the embryo just starts to grow out of the hole and the zona stays thick.
Here’s an example of a embryo that has a thick zona (on the left), but you can see it hatching (on the right). The hole is in the middle and you can see where it’s squeezing out:

In this case the embryo was likely assisted hatched to prepare for PGT-A, because the zona is still thick.
How clinics grade the expansion for biopsied embryos can be incredibly variable!
Some might keep it simple and call them a 5, because it’s hatching. Others might only reserve the expansion 5 title for those that are naturally hatching (and not assisted). In this case they can get creative with how they determine the expansion. If there’s not many hatching cells, they might call it a 3, if there’s more it might be a 4, and if there’s a lot then it might be a 5.
Thankfully, there is no variability in a 6. A 6 is hatched out and that’s it.
Inner Cell Mass (ICM)
The ICM is the part of the embryo that develops into the fetus and is indicated by the first letter in the embryo grade (the “A” in 4AB).
ICM quality depends on the number of cells and how compacted they are. It’s kind of like the way you’d make a good snowball. You want a good amount of snow, and you want it tightly packed, otherwise it will fall apart.

As you may have guessed from the last section on the variability of the expansion grade, there can be variability in the ICM grade.
Besides the Gardner system, another grading approach is the ACE/NEQAS system, which is widely used in the UK and Europe. This system adds a “D” grade alongside A–C. A “D” means there are no visible ICM cells, or the visible cells are degenerating (dying — they look darker and wrinkled or compacted). In the Gardner system, these same embryos would be graded as “C,” so a “D” in ACE/NEQAS represents a very poor quality ICM.
Some clinics don’t even use the letter systems and have numbers or a + and – system. Furthermore, what’s an A to one embryologist may be a B to another (even from the same clinic!).
Trophectoderm
The trophectoderm develops into the placenta and is indicated by the second letter of the blastocyst grade (the “B” in 4AB).
Like the ICM, trophectoderm quality depends on the number of cells and how cohesive and packed together they are. The trophectoderm is like the igloo which needs many blocks of ice that fit together well otherwise it may fall apart.

With the ACE/NEQAS system, a “D” graded trophectoderm means there are few cells that are large, flat or dying (degenerating). In the Gardner system, these same embryos would be graded as “C,” so a “D” in ACE/NEQAS represents a very poor quality trophectoderm.
Again, the trophectoderm grade can vary depending on the embryologist. What’s an A graded trophectoderm to one embryologist, may be a B to another (even from the same clinic).
ICM and trophectoderm grading for early blastocysts
Many centers don’t give a quality grade for the ICM or trophectoderm for early blastocysts (those with expansion 1 or 2). This is because the embryos are still developing their ICM and trophectoderm so it can be hard to tell what their quality is. In this case, you might just see a “1” or “2” as the grade and no letters.
Once the embryo becomes a 3 or more, it’s much more accurate to grade the ICM and trophectoderm.
Are fully hatched embryos more fragile?
This is a question sometimes asked when people have a fully hatched (expansion 6) embryo. Since the zona is gone, some worry that these embryos are more exposed and more fragile.
I haven’t found too much research on it but Kirienko et al. (2019) did a study where they transferred artificially hatched embryos along with unhatched embryos. They didn’t find any differences in success rates (implantation rate, pregnancy, miscarriages).
If you want to check out the full summary you can check my post Is a fully hatched embryo more fragile than an unhatched embryo?
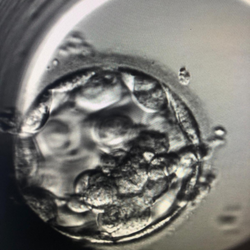
Embryo compaction
Blastocysts can sometimes look a bit “compacted” or squished. Here’s an example:

Blastocysts are filled with water and sometimes this water escapes as the embryo grows in size. Remember, they’re like water balloons, and sometimes this balloon can “pop” to release the water.
Blastocysts actually expand and contract (or collapse/compact) as a part of their normal development. Some think it may be a way for the blastocyst to help the hatching process.
Embryos can be artificially compacted, or collapsed, by using a laser. This is usually done before freezing to remove the water from inside the embryo. It’s important to do this because when water freezes it can form sharp ice crystals that can damage the embryo. Darwish 2016 found that embryos that were artificially collapsed before freezing had improved survival compared to those that weren’t.
After thaw, the embryo will re-expand and this shouldn’t take more than a couple of hours. Kinzer 2011 found that embryos that re-expanded more than 40% within two hours post thaw had a higher chance of implanting (~36% implantation vs ~10%).
Embryos that are compacted, or collapsed, are difficult to evaluate for their quality because the ICM and trophectoderm may not be clearly shown. You can appreciate this by taking another look at the picture above and noticing how the ICM (around 9 o’clock) is pretty hard to make out when the embryo is collapsed.
If you want to learn more about embryo compaction and how success rates might be impacted, check my post What is Embryo Compaction?
What are “cytoplasmic strings?”
Cytoplasmic strings are string-like structures that can be seen in an embryo photo. These strings connect the ICM and the trophectoderm cells, and it’s not clear what their function is.
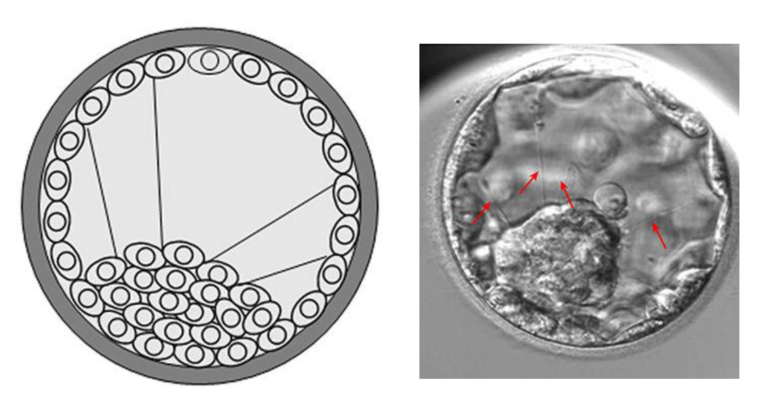
Ma et al. (2022) found that these strings are more commonly seen in good quality embryos, and more strings indicated a higher chance for pregnancy or live birth rate.
You can read more about cytoplasmic strings in my post Improved live birth rates in blastocysts with “cytoplasmic strings.”
How blastocyst embryo grades are reported
The usual way is by using the Gardner system, as I explained above. This uses a number followed by two letters, where the number indicates the embryo’s expansion (from 1-6) and the quality (A, B or C) of the inner cell mass (ICM) and trophectoderm.
Here’s a handy quick guide to help you put it all together:

As mentioned, some clinics might use “D” in addition to ABC, while others may use A-F. Others may use “grade I” in place of “A” or use a “+” or “-” sign where an A+ would be a perfect grade.
Other clinics might convert the letters to numbers. A 4AA would be represented as 4-3-3, a 4CC as 4-1-1.
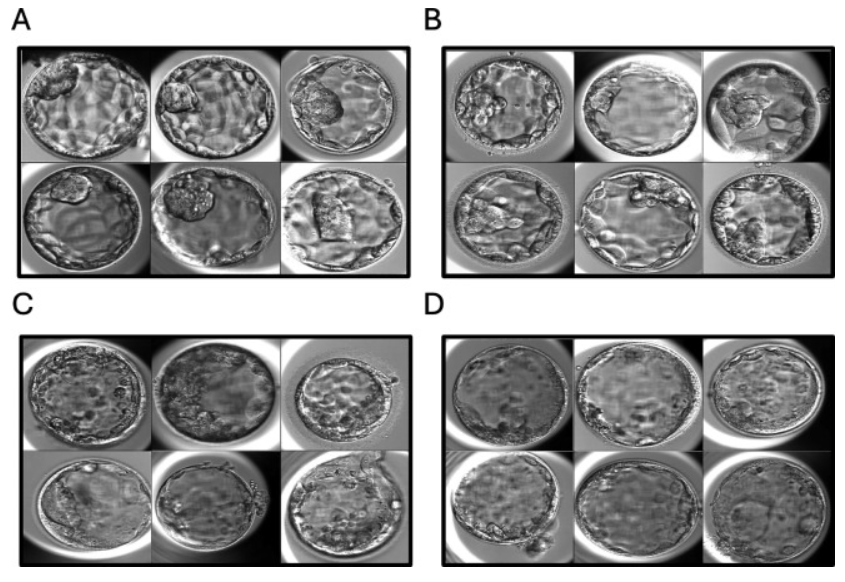
Day 5 (blastocyst) embryo grades and pictures
Here are some pictures of day 5 embryos (blastocysts) and their grades. This is from my Embryo Gallery where I post pictures of submitted embryo photos and their grades from my supporters. Check it out to see a lot more!






Blastocyst Embryo Grading and Success Rates
What’s more important for an embryo’s grade: Expansion, ICM, or trophectoderm?
What’s more important, the expansion of the embryo, the ICM, or the trophectoderm? In other words is a 5BB better than a 3AA? Or is a 3BA better than a 3AB?
Interestingly, like most things in IVF, the answer is not clear!
Morbeck (2017) did a review of 8 studies that drew conclusions based on whether the ICM, trophectoderm, or expansion were the most predictive for implantation:
- 2 studies showed the ICM was predictive.
- 4 studies showed the trophectoderm was predictive.
- 1 study showed embryo expansion was predictive.
- 1 study showed that none of the above were predictive!
This is the kind of thing that should be deferred to the clinic. Each clinic will have their own recommendation on what’s better. Some may prioritize the ICM quality over the trophectoderm quality, while others may look more at the expansion.
Embryo Quality
Generally, good quality embryos have a higher chance for live birth than fair quality, which have a higher chance than poor quality embryos.
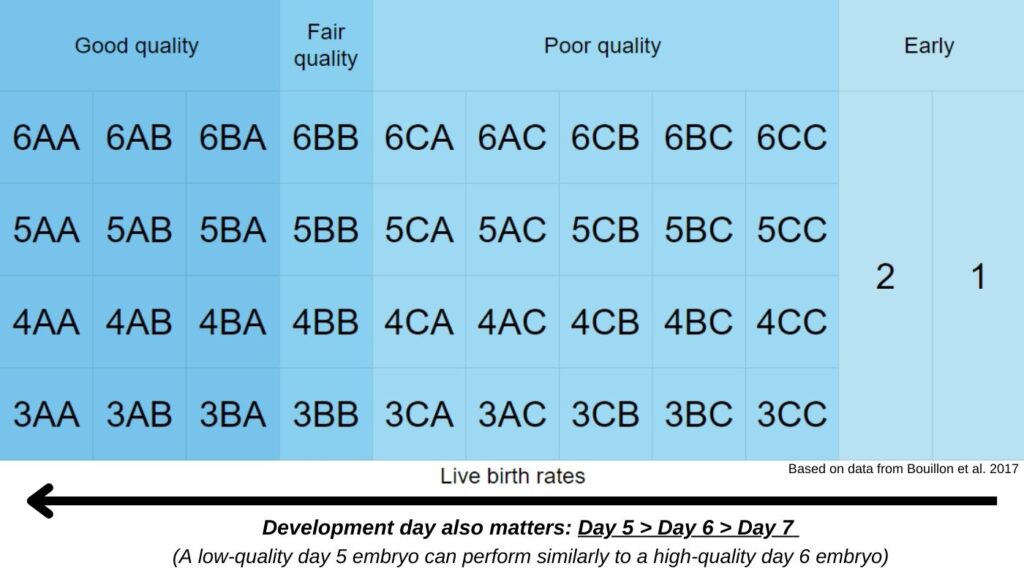
Bouillon et al. (2017) compared the transfer of a single day 5 early blastocyst, or expanded/hatching/hatched good, fair or poor quality embryos:
- Good quality embryos included embryo grades 6AA, 6AB, 6BA, 5AA, 5AB, 5BA, 4AA, 4AB, 4BA, 3AA, 3AB and 3BA, which had a live birth rate of 46.8%.
- Fair quality embryos included embryo grades 6BB, 5BB, 4BB and 3BB, which had a live birth rate of 39.0%.
- Poor quality embryos included embryo grades 6CA, 6AC, 6CB, 6BC, 6CC, 5CA, 5AC, 5CB, 5BC, 5CC, 4CA, 4AC, 4CB, 4BC, 4CC, 3CA, 3AC, 3CB, 3BC and 3CC, which had a live birth rate of 34.1%.
- Early blastocysts included embryo grades 1 and 2, which had a live birth rate of 28.9%.
- There was no statistical difference in miscarriages (13.7% vs 14.6% vs 19.1% vs 18.7%).
- There was no differences in ectopic pregnancies, preeclampsia, preterm birth, low birth weight, neonatal complications, congenital malformations and other outcomes.
- Female age ranged from 30.7 to 32.1.
Note: This study didn’t indicate the number of each type of embryo for these groups. So while a 3CC is indicated here as having a 34.1% live birth rate, that’s part of a larger group of poor quality embryos which may have had more 5ACs or 4BCs for example that may have tilted the success rates. This study also only included day 5 embryos, but other studies have shown that the day of development matters, with day 5 blastocysts tending to perform better than day 6 and 7.
Oron et al. (2014) looked at single embryo transfers of 849 blasts between 2008-2012 in women <40 years of age. Good quality (≥3BB) and poor quality (<3BB) were evaluated:
- Good quality blasts (≥3BB) a live birth rate of 41% was achieved
- Poor quality (<3BB): 26%.
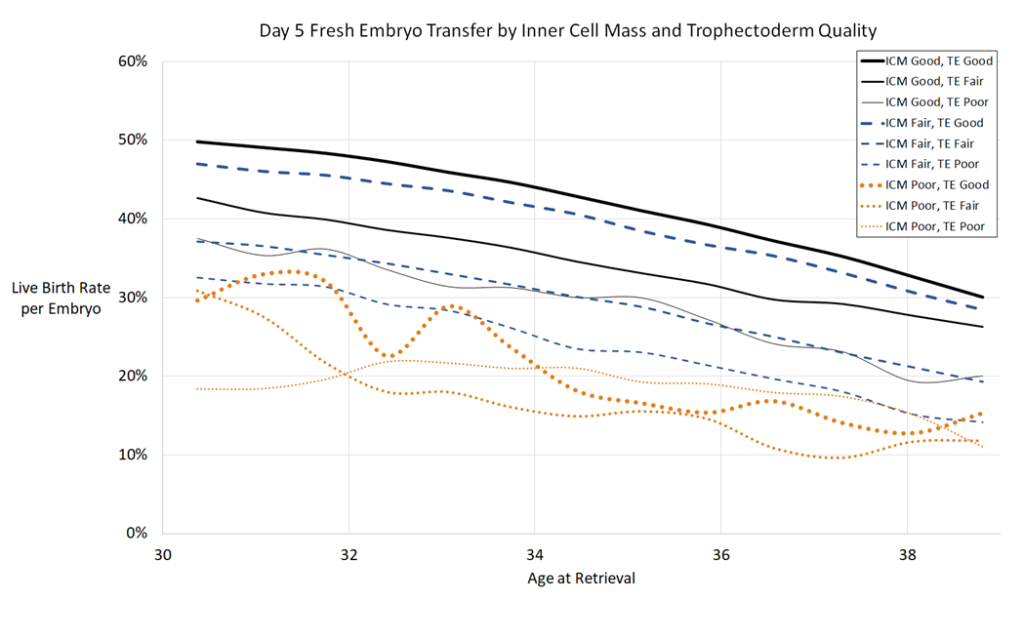
Awadalla et al. (2022) created models to predict live birth rates based on 223,377 embryo transfers in the US. You can see the graph below that shows how different blastocyst ICM and trophectoderm qualities correspond to live birth rates:

This study also looked at frozen transfers and how the embryo’s expansion plays into this. Generally early blasts have a lower success rate compared to expanded blasts, which have a lower success rate compared to hatching blasts. I have the full summary of this study on my post Predicting live birth rates, multiples based on 223,377 transfers.
I really like that graph above because it also shows how age plays into things. We’ll talk about this in more detail below, but an embryo’s quality is only one part of what dictates success rates: age is very important also!
One meta-analysis ranked every possible embryo grade for its ability to lead to a live birth. You can see this below, with the 5AA having the highest potential for live birth and the 1CC the lowest:
5AA, 4AA, 6AA, 5AB, 3AA, 5BA, 4AB, 2AA, 4BA, 6AB, 5AC, 3AB, 5CA, 6BA, 1AA, 5BB, 4AC, 3BA, 4CA, 2AB, 4BB, 2BA, 6AC, 6CA, 3AC, 5CB, 6BB, 1AB, 3CA, 5BC, 3BB, 1BA, 4CB, 2AC, 4BC, 2CA, 2BB, 6CB, 5CC, 6BC, 1AC, 3CB, 3BC, 1CA, 1BB, 4CC, 2CB, 2BC, 6CC, 3CC, 1CB, 1BC, 2CC, 1CC.
They also ranked every grade based on its chance of miscarriage (5AA has the lowest chance and 2CC has the highest chance):
5AA, 5BA, 5AB, 1AA, 3AA, 4AA, 6AA, 5BB, 1BA, 3BA, 5CA, 1AB, 3AB, 4BA, 6BA, 4AB, 5AC, 6AB, 1BB, 3BB, 5CB, 1CA, 3CA, 2AA, 4BB, 5BC, 6BB, 4CA, 6CA, 1AC, 3AC, 2BA, 1CB, 3CB, 2AB, 4AC, 6AC, 1BC, 3BC, 4CB, 5CC, 6CB, 2BB, 2CA, 4BC, 6BC, 1CC, 3CC, 2AC, 2CB, 4CC, 6CC, 2BC, 2CC.
You can read more about this study in my post Study evaluates which embryo grades predict IVF success.
Poor quality embryos work – check your clinic’s policy on discarding them
You’ll notice from above that poor quality embryos may have reduced implantation rates and higher risks of miscarriage compared with higher graded embryos. Because of this, some clinics have minimum quality thresholds for transfer. It’s important to check with your clinic about their policies when planning a cycle.
There’s quite a bit of data I’ve compiled about these embryos, and you can check it out on my Grade C (poor quality) embryo success rates post. Here’s a couple of studies:
- Bouillon et al. (2017) (more details in the previous section): C grade live birth rates were 34.6% compared to 39.0% (grade B) and 46.8% (grade A) and had similar obstetric and perinatal outcomes (ie no increase in miscarriage) (average age 30-32).
- Van den Abbeel et al. (2013): reduced live birth (from 45% for A grade to 20% for C grade) (ages <35)
As we’ll see, day 5 embryos tend to perform better than day 6 embryos, and He et al. (2023) found that poor quality day 5 embryos had comparable outcomes to day 6 good quality embryos. This is an interesting comparison because while clinics would transfer a good quality day 6 embryo, some would hesitate with a poor quality day 5 embryo. Check the full summary in my post Comparable outcomes with good quality day 6 and poor quality day 5 embryos.
💡 Want to see real success stories with lower-grade embryos?
Check the IVF Success: Poor quality embryo collection from the Uterine Wall of Fame, which features a growing collection of IVF success stories submitted by people who have been through it themselves.
Timing of blast development: Day 5, 6 or 7?
Normally embryos become blastocysts on day 5, but sometimes embryos take longer to develop and may become a blastocyst on day 6, day 7 or even day 8.
Embryos can also develop faster and become blastocysts on day 4!
Ferreux et al. (2018) found that day 5 embryos performed better than day 6 regardless of grade (29.6% live birth vs 17.0%).
One study compared grades with day 5 and day 6 embryos, and they found that a poor quality day 5 embryo had similar live birth rates compared to a good quality day 6 embryo! They also found no differences in neonatal outcomes, so day 6s didn’t lead to more preterm births or low birth weights (in other words they led to babies that were as healthy as day 5 blastocysts). You can read more about this study in my post Comparable outcomes with good quality day 6 and poor quality day 5 embryos.
Du et al. (2018) found live birth rates from day 7 embryos were about half of day 5 and day 6 (~25% vs ~45%) with no differences in low birth weight, malformations or early neonatal death.
Giulia et al. (2022) compared the outcomes of day 5, 6 and 7 blastocysts that were tested for PGT-A (and were euploid). They found increases in miscarriage rates from day 5 to day 7, with decreases in live birth rate. You can see this below:
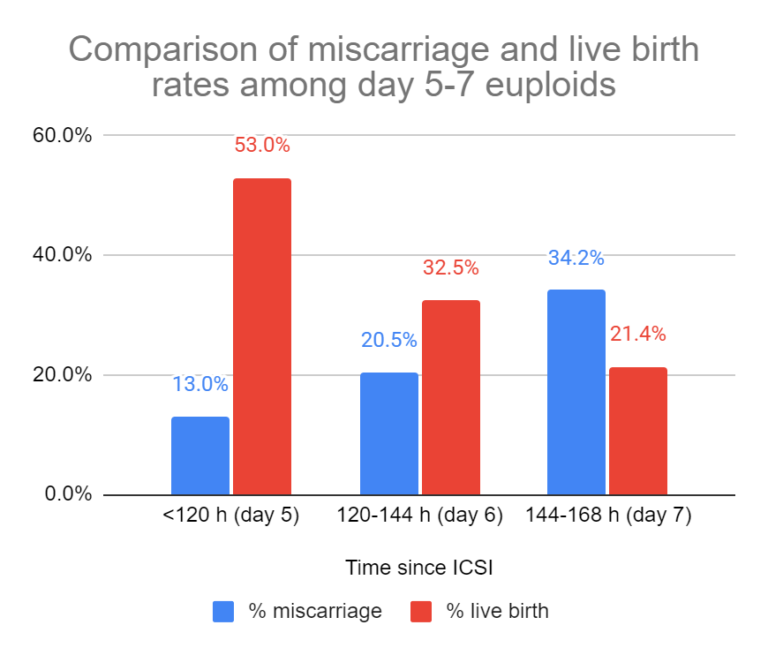
If you wanted to read more about this last study you can check my post Transfer of day 7 embryos a viable option.
Huang et al. (2020) found no difference in gestational age, birth weights, complications, and other outcomes among nearly 100 births from day 7 embryos compared to day 5 or 6.
Another study compared outcomes after transferring a single day 4, 5, 6 or 7 blastocyst. Yes, embryos can be a bit quick to develop and become a blastocyst on day 4!
- Day 4 blasts had the highest chance of live birth (43.4%).
- Day 5 live births were 33.6%.
- Day 6 was 13.2%.
- Day 7 was 4%.
There weren’t many day 7 transfers though, so these results weren’t really reliable for this group. They also looked at how this changed with age, which was interesting. To read the full study, check my post Study evaluates the potential of day 4, 5, 6 and 7 blastocysts.
Sometimes it’s possible to go even beyond day 7 — to day 8. In 2021, the first reported case of a day 8 healthy live birth was reported. It was PGT-A tested and good quality. Typically, labs won’t culture embryos to day 8, but “good quality [PGT-A tested] embryos after 8 days of culture should be considered for embryo transfer,” the researchers reported.
Day 7 embryos work – check your clinic’s policy on discarding them
You’ll notice from above that day 7 embryos may have reduced implantation rates and higher risks of miscarriage compared with day 5 or 6. Because of this, some clinics don’t culture to day 7. It’s important to check with your clinic about their policies when planning a cycle.
Giulia et al. (2022) compared the outcomes of day 5, 6 and 7 blastocysts that were tested for PGT-A (and were euploid). They found that if they stopped culturing at day 6 and didn’t culture embryos to day 7, there would be a:
- 10.6% reduction in patients with blastocysts
- 7.3% reduction in patients with euploids
- 4.4% reduction in patients with a live birth
In other words, if these patients didn’t culture to day 7, about 10% wouldn’t have any blastocysts to transfer!
If you wanted to read more about this study you can check my post Transfer of day 7 embryos a viable option.
💡 Want to see real success stories with day 7 embryos?
Check the IVF Success: Day 7 embryo collection from the Uterine Wall of Fame, which features a growing collection of IVF success stories submitted by people who have been through it themselves.
How many day 3 embryos make it to blastocyst? Do embryo grades matter?
As an embryo develops to day 3, there’s a chance the embryo will continue development, or will stop developing and arrest. We’ll talk more about why embryos arrest in the next section, but first let’s discuss how often a day 3 embryo progresses into a blastocyst, or blastocyst conversion as it’s called.
Like everything with IVF, there’s a certain probability attached to blastocyst conversion. Good quality day 3 embryos tend to have a higher chance of making it to blastocyst. Alikani et al. (2000) found that the highest rate of blastocyst conversion was with day 3 embryos with 7-9 cells and <15% fragmentation (~35%-40%). This was reduced to <10% with <5 cells, or about 10% with >25% fragmentation.
Blastocyst conversion is dependent on age, and older women tend to produce fewer blastocysts. You can see this in the graph below from Romanski et al. (2022), which looks at the % of fertilized eggs that go on to form blastocysts:
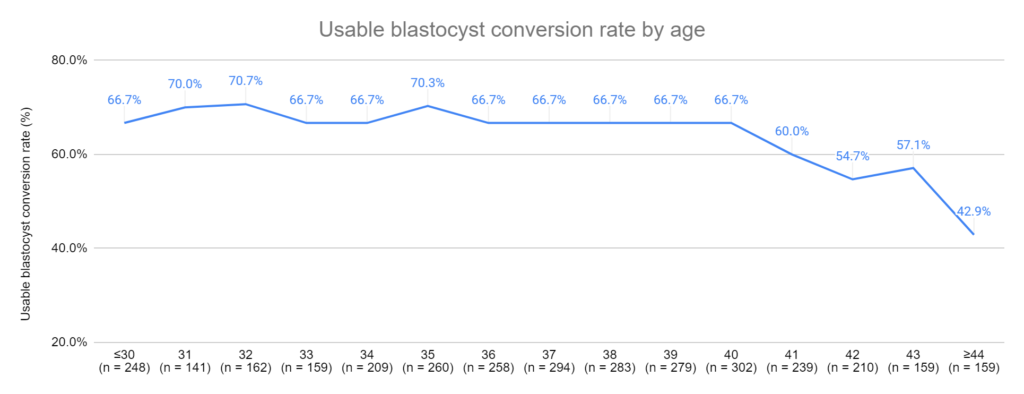
You can read the full study in my post Age-specific blastocyst conversion rates and other IVF outcomes in good prognosis women. They also examine how many eggs people get with increasing age, the number that are mature, the number that fertilize, etc. This study is very interesting!
Another more personalized way of figuring out how many blastocysts will develop is to use the nomogram developed by Jin et al. (2021). A nomogram is kind of like a calculator that you can use to predict something, and this study’s nomogram predicts how many blastocysts will develop. You can check it out in my post Predicting how many day 3 embryos make it to blastocyst.
Why do embryos arrest, or stop developing, and don’t become blastocysts?
Sometimes embryos don’t progress to blastocyst at all, and “arrest” at day 3. This happens because, for one reason or another, an embryo doesn’t have “the right stuff” to progress to day 5 and become a blastocyst.
Becoming a blastocyst requires a massive shift in development. The embryo’s DNA comes together after the sperm and egg DNA combine during fertilization, but the resulting embryo’s DNA (genome) isn’t ready yet. The sperm’s DNA is still highly compacted and “decondensation” needs to occur, as well as steps involved in “reprogramming” the embryo’s DNA so that genes involved in embryo development are activated. This process usually takes a few days. In this time, the embryo can’t yet use it’s genome to make the proteins it needs to divide and grow, so it uses stored factors that were left behind in the egg to develop.
Some embryos arrest because they can’t switch from the stored maternal egg factors to the embryo’s genome, while others have metabolic issues. I get into this in more detail in the post Genetic analysis of arrested embryos reveals 3 distinct types.
Embryos can also arrest for different reasons:
- Aneuploidy (not having the right number of chromosomes)
- Mutations in key genes
- Problems with mitochondria (the “batteries” of the cell)
- DNA fragmentation in sperm
- Unfavorable lab conditions (ie. air quality)
I cover this all in detail in my post on Embryo arrest.
💡 Want to see real success stories with people who experienced a high degree of embryo arrest?
Check the IVF Success: Embryo arrest collection from the Uterine Wall of Fame, which features a growing collection of IVF success stories submitted by people who have been through it themselves.
Do embryos grades matter after PGT-A?
One thing I hear often is that embryo grading doesn’t matter if PGT-A is done and the embryo is euploid. This isn’t accurate!
Zhao et al. (2018) looked at euploid embryos in women <35:
- Graded as excellent (AA) or good (AB or BA) = 50% live birth
- Average (AC, CA or BB) = 42% live birth
- Poor (BC or CB) = 25% live birth
So grading appears to give euploids a ranking order for transfer, just like what we’ve seen with untested embryos. Good quality euploids tend to perform better than fair quality, which tend to perform better than poor quality.
Other studies have found a similar impact of grades on euploids, including the impact of day 5, 6 and 7 (reviewed in my post on PGT-A (PGS) success rates).
Why did my embryo grade change after it was thawed?
Occasionally you might find that your embryo’s grade changes. This is usually after an embryo is frozen with one grade, and then gets a different grade after it was thawed. In some cases the expansion might change, or even the embryo’s quality.
This can happen because the embryo can develop significantly in the time between thaw and transfer. Embryos are normally thawed in the morning but your transfer might not be until later in the day, which gives it time to continue developing.
Another reason is that embryo grading is subjective, and one embryologist might give it a different grade compared to the original embryologist who graded it. I have more information on this below.
Why embryo grades do not matter
So if you’ve gotten this far in this guide, it should be clear to you that embryo grades matter. I’ve heard people describe embryo grading a “just a beauty contest,” which is a bit misleading. There’s a reason embryos are graded. It’s used as a way to rank embryos for transfer, with the better quality embryos having a higher chance of implanting compared to the lower quality embryos.
This is demonstrated by this embryo grading chart below (which I discuss in more detail above!):

But this doesn’t mean that an embryos grade will dictate whether or not the embryo will implant. In fact, it’s fairly common for transfers of good quality embryos to result in implantation failure.
Maternal age
The statistics covered in this guide are highly dependent on maternal age, specifically the age of female at the time of egg retrieval. Older women tend to produce more aneuploid eggs, which result in aneuploid embryos. Aneuploid embryos tend to not implant, or fail to have sustained implantation.
According to Goto et al. (2011), younger women <33 years old with high quality blastocysts have a 59.9% chance of live birth, while older women >38 years old with high quality blastocysts have a 32.6% of live birth. This is because the eggs from older women are more likely to produce aneuploid embryos that have a lower chance of achieving a live birth.
We can see how age plays a role in the graph below, based on the Awadalla et al. (2022) study shown earlier:
(I have the full summary of this study on my post Predicting live birth rates, multiples based on 223,377 transfers).
Implantation failure
Even the best of the best, a PGT-A tested euploid embryo, doesn’t always work! Pirtea et al. (2020) found that good prognosis women who transferred up to 3 euploid embryos (one at a time, for a total of three transfers) had a cumulative live birth rates of 92.6% by the third transfer. So about 10% of good prognosis women, who transfer up to 3 euploids, will still fail to achieve a live birth.
(I cover this study, and others in my post How many failed embryo transfers is too many?)
Craciunas et al. (2019) states “It is estimated that embryos account for one-third of implantation failures, while suboptimal endometrial receptivity and altered embryo–endometrial dialogue are responsible for the remaining two-thirds”.
Besides the impact of the embryo, why does implantation failure or miscarriage occur? There are a lot of reasons:
- Lifestyle
- Infections or endometritis
- Problems with the vaginal or endometrial microbiota
- Anatomical issues (like polyps or fibroids)
- Thrombophilia
- Immunological issues (autoimmunity, NK cells, T regulatory cells, HLA mismatching)
- Endometrial receptivity
- Undiagnosed genetic mutations
- The doctor’s and embryologist’s success rates
I cover all of these points in my post Why do embryos in IVF fail to implant or miscarry?
Embryo grading is subjective
If you remember from my earlier section on blastocyst grading, the expansion, ICM and trophectoderm are the three features that are graded. Embryologists can have a different opinion on what makes the qualities of these features good, fair or poor.
Storr et al. 2017 found that while 10 experienced embryologist were able to consistently choose the best embryo for transfer, they weren’t consistent with grading.
There’s likely more differences between clinics, because they may have different ways of training their embryologists, but even embryologists from the same clinic may have different opinions on grades. It’s important for embryologists to receive regular training to ensure consistency, but this isn’t practiced everywhere.
Conclusions
Embryo grading is used during IVF to rank embryos for transfer after evaluating different parts of the embryo.
For cleavage stage embryos (day 2 or 3 embryos), embryo grading is mainly based on the number of cells and the amount of fragmentation the embryo has.
For blastocyst stage embryos (day 5, 6 or 7), embryo grading is based on the embryo’s size (expansion) and the quality of the inner cell mass (ICM) and trophectoderm.
By transferring these embryos to patients, different studies have shown that lower quality embryos tend to result in fewer live births compared to high quality embryos.
Embryos of all qualities have been shown to result in live births, even poor quality embryos or blastocysts that develop on day 7, and it’s important to discuss your clinic’s policies when planning a cycle.
Embryo grades aren’t the only variable that affects live birth rates. Age is a critical factor as well as the endometrial environment where the embryo implants. Embryo grading is very subjective, and not all embryos will grade embryos the same.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.