Researchers in a 2023 study performed a randomized controlled trial on the use of assisted hatching on patients with recurrent implantation failure, and found found no improvement in cumulative live birth rates, while miscarriage rates decreased.
Assisted hatching involves using a laser to make a small hole in the zona of the embryo, and is believed to help the embryo hatch. This might be particularly helpful in patients with recurrent implantation failure (RIF).
Curfs et al. (2023) performed a randomized controlled trial (RCT) to see if assisted hatching can improve the cumulative live birth rate in women with RIF. In this study, the cumulative live birth rate is the total live birth rate after fresh and additional frozen transfers from a single ovarian stimulation cycle.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- This was a double-blind, RCT that involved 600 participants between 2012 and 2017 at five IVF clinics in the Netherlands.
- Patients were aged 18-42 and had RIF.
- RIF was defined as either 1) Two consecutive failed fresh embryo transfers; or 2) One fresh transfer that failed, followed by two failed frozen transfers using embryos from the same cycle.
- For all participants, they had a single ovarian stimulation cycle followed by a fresh transfer involving 1-2 day 3 embryos. If this first transfer failed, patients could perform additional frozen transfers.
- Embryos in the assisted hatched group were hatched 1 hour before transfer.
In terms of baseline characteristics, there were no differences between the groups’ age, duration of infertility, diagnosis, use of IVF or ICSI, number of eggs retrieved, number of embryos transferred, quality of embryos transferred, and more.
For the assisted hatching + no assisted hatching groups, there were originally 300+300 patients enrolled, with 277+282 having an ovarian stimulation cycle, 264+271 having a fresh transfer, followed by 98+92 with a second frozen transfer. In the end there were 22+26 participants with extra embryos still available.
This study is meant to replicate what would be seen in a real clinic: patients have an egg retrieval, transfer a fresh embryo, and perform additional frozen transfers until they either have a live birth, or have no embryos left. The primary outcome of this study was the cumulative live birth rate. Secondary outcomes included various pregnancy and neonatal outcomes.
Pregnancy outcomes with assisted hatching
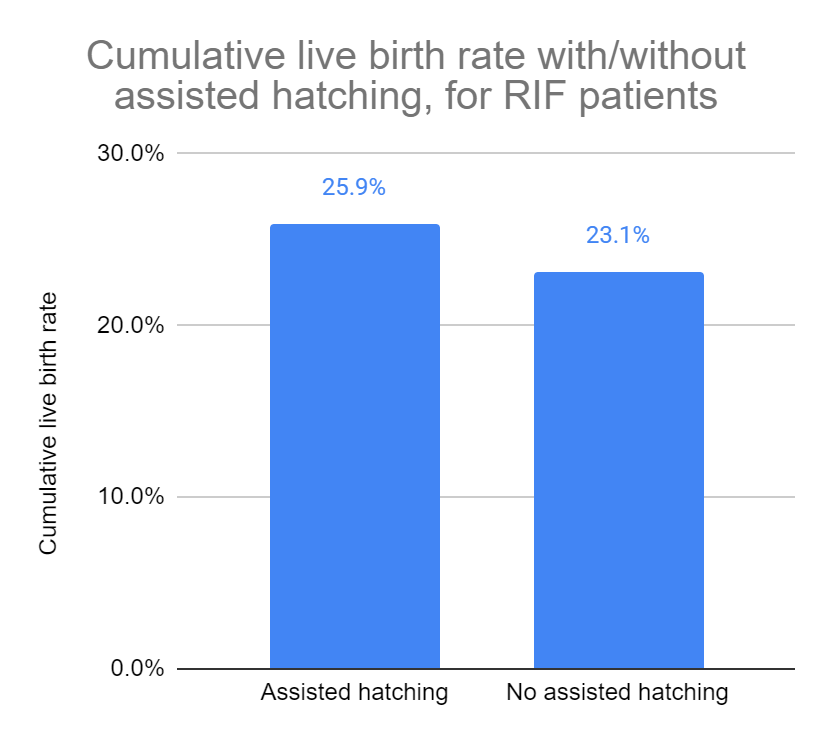
There was no difference in the cumulative live birth rate for patients that had assisted hatching vs those that didn’t (25.9% vs 23.1%, relative risk [95% CI]: 1.125 [0.847-1.494]).
There were also no differences in the cumulative pregnancy rate, or cumulative ongoing pregnancy rate.
When they only considered the first fresh transfer, there were no differences in the pregnancy, ongoing pregnancy or live birth rate. They evaluated this per couple, per egg retrieval, and per embryo transfer.
For their secondary outcomes, which hold less weight than the primary outcome, they found:
- Assisted hatching reduced miscarriage rates by about half (17.3% vs 34.6%, relative risk [95% CI]: 0.532 [0.296-0.992]).
- No difference in multiple pregnancies.
- No difference major/minor malformations in the child.
- No difference in chromosomal aberrations in the child.
They also did a number of subgroup analyses, including where they compared outcomes for women 34 or younger vs those older than 34. They found that miscarriage rates were lower for women 34 or younger, but not for older women (14.9% vs 34.0%, relative risk [95% CI]: 0.184-0.985]). So the benefit of assisted hatching in reducing miscarriage only benefited women 34 or younger in this study.
They didn’t find any other differences in the subgroup analysis (based on age and history of failed transfers for cumulative live birth, fresh transfer live births and miscarriages).
Conclusions
This study found no difference in the cumulative live birth rate (which included live births from the first fresh transfer and subsequent frozen transfers). This is consistent with previous research.
Miscarriage rates were lower when assisted hatching was done, which was only found in women 34 and younger (and not in the older participants).
The authors warn that their study wasn’t large enough to assess miscarriage rates, so this result should be interpreted with caution. Previous studies have found no difference with miscarriage rates, including a recent meta-analysis which I review here. Based on this, the authors don’t recommend assisted hatching for decreasing miscarriage rates.
This study also found no differences in pregnancies, multiple pregnancies, or congenital malformations in the child.
Previous studies, including the meta-analysis that I review here, found an increase in the rate of multiples with assisted hatching. Since there were only a small number of multiple pregnancies in this study, it’s hard to draw conclusions.
Based on this, the authors recommend that assisted hatching is offered only with an understanding that there isn’t any evidence for a benefit, at zero cost, and ideally in a research setting.
A limitation of this study is that there isn’t a universally accepted definition of recurrent implantation failure, and there may be different results with patients that have a history of more failed transfers.
The European Society of Human Reproduction and Embryology (ESHRE) recently recommended against the use of assisted hatching, for the general public, citing no improvements in live birth rates and a possible increase in monozygotic twinning (see my post for more info Evidence-based recommendations from ESHRE for 27 IVF add-ons).
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Meta-analysis examines the use of assisted hatching on IVF outcomes
Meta-analysis examines the use of assisted hatching on IVF outcomes
 Evidence-based recommendations from ESHRE for 27 IVF add-ons
Evidence-based recommendations from ESHRE for 27 IVF add-ons
 Meta-analysis examines the use of embryo glue on IVF outcomes
Meta-analysis examines the use of embryo glue on IVF outcomes
 Clinical trial finds no benefit with time-lapse (embryoscope)
Clinical trial finds no benefit with time-lapse (embryoscope)
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer
 Growth hormone (omnitrope) increases number of eggs retrieved in updated meta-analysis
Growth hormone (omnitrope) increases number of eggs retrieved in updated meta-analysis