
Researchers in a 2024 study performed a network meta-analysis and combined the results of 23 studies involving 7 different growth hormone (omnitrope) protocols in poor responders. None of the protocols improved clinical pregnancy rates, but one protocol showed improvements in IVF outcomes like the number of eggs retrieved.
Women with poor ovarian response (POR) don’t make many eggs after ovarian stimulation, and one way to overcome this is to use growth hormone (GH aka omnitrope). There are a variety of treatment protocols for GH during IVF, and this meta-analysis aimed to determine which one works best in terms of leading to a clinical pregnancy.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- There were 15 randomized controlled trials (RCTs) and 8 cohort studies included in this meta-analysis, including a total of 4,889 cycles.
- All patients were diagnosed with POR, usually by the Bologna criteria (check the glossary for POR). Women with POR don’t produce many eggs after ovarian stimulation.
- These 23 studies included 7 different GH protocols (shown below). Note that the follicular phase is days ~1-14 of the menstrual cycle (or the phase before the egg retrieval), the luteal phase is days ~14-28 (or the phase after the egg retrieval), and the hCG day is the day of hCG trigger.
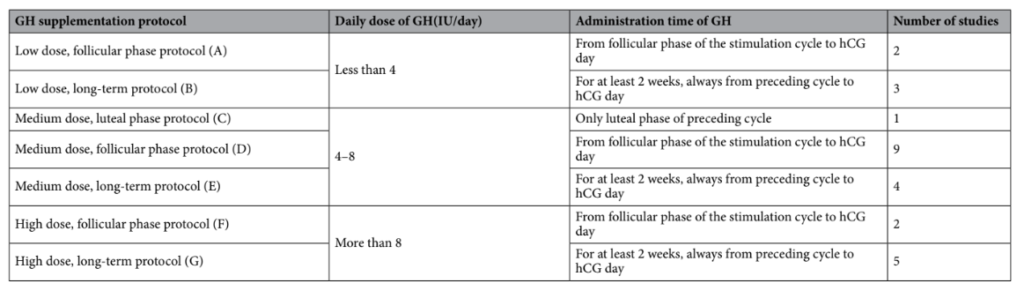
- For each protocol A-G, the control used was either a placebo or no GH.
- A “network” meta-analysis was used, which lets you combine studies that have different treatment protocols that aren’t directly compared. Check the glossary for “meta-analysis” for more info.
- The primary outcome was the clinical pregnancy rate.
No improvement in clinical pregnancy rates with growth hormone
They found no difference in clinical pregnancy rates for POR patients using GH (protocols A-G) vs the control. You can see the odds ratios below, with the corresponding 95% CI, which show that none of them are statistically significant:
- Protocol A 1.33 (0.53, 4.25)
- Protocol B 3.67 (0.94, 18.09)
- Protocol C 0.94 (0.31, 3.11)
- Protocol D 1.69 (0.96, 3.48)
- Protocol E 1.31 (0.49, 2.67)
- Protocol F 5.02 (0.53, 175.42)
- Protocol G 1.44 (0.55, 2.35)
Some improvements in IVF outcomes with growth hormone
Besides clinical pregnancy, the researchers also looked at a number of different IVF outcomes, some of which were improved after GH with certain protocols (in bold, with the corresponding 95% CI):
- Total gonadotropin dose (decreased with protocol D vs the control by 764.31 IU [-1519.71 – -12.46])
- Number of retrieved eggs (increased with protocol D vs the control by 1.19 [0.29-2.00])
- Number of retrieved mature eggs (increased with protocol D vs the control by 1.82 [0.68-2.99]; increased with protocol G vs the control by 1.75 [0.19-3.31])
- Number of fertilized embryos (no difference)
- Serum E2 levels on hCG trigger day (no difference)
- Endometrial thickness on hCG trigger day (increased with protocol D vs the control by 0.44 mm [0.18-0.68]; increased with protocol E vs the control by 0.64 mm [0.27-1.10])
- Live birth rate (no difference)
So the total gonadotropin dose decreased*, the number of retrieved (mature or not) eggs increased and the endometrial thickness on hCG trigger day increased with protocol D. Protocols G and E also had some benefit on the number of mature eggs and endometrial thickness.
*In patients with POR, who don’t produce many eggs after ovarian stimulation, a higher amount of gonadotropins like FSH are often administered. This result shows that GH lowered the amount of gonadotropins needed for a cycle, which shows that GH improved ovarian response.
Clinical pregnancies increased with growth hormone in certain subgroups
The researchers then did a subgroup analysis using only the data from studies that used protocol D. They wanted to see if there were any patient groups in these studies where the clinical pregnancy rate was higher. They looked at the following groups:
- Patients grouped by diagnostic criteria (Bologna, Poseidon, self-defined).
- Patients grouped by study design (RCTs, non-RCTs)
- Patients grouped by ovarian stimulation protocol (GnRH antagonist ultrashort, GnRH agonist short, GnRH agonist long, multiple protocols).
- Patients grouped by region (the study took place in Europe, Asia or Africa).
They found that if they only included RCTs, then the clinical pregnancy rate increased by 76% (odds ratio [95% CI]: 1.76 [1.12-2.76], based on 6 studies and 487 participants).
They also found that studies that took place in Africa showed an improvement in clinical pregnancy rate by 65% (odds ratio [95% CI]: 1.65 [1.03-2.65], based on 3 studies and 401 participants). The researchers noted that this group had more recent RCTs, which likely led to the results seen.
There were no differences for protocol D and clinical pregnancy rates for the other subgroups.
Conclusions
This meta-analysis found no improvements in clinical pregnancy after using any of the 7 GH protocols.
Different meta-analyses have been done looking at GH with mixed clinical pregnancy results, including the most recent one that I reviewed that showed a benefit. You can find links to the other studies below.
The most common protocol involved administering 4-8 IU/day during the follicular phase of the ovarian stimulation cycle, until the hCG trigger.
They did find improvements in some outcomes when using this protocol, in terms of a reduced total gonadotropin dose, increased number of retrieved eggs, increased number of mature eggs and a thicker endometrium.
So even though they didn’t find an improvement in clinical pregnancies (or live births), they did find an increase in the number of eggs retrieved. This could potentially lead to more embryos for a patient, and lead to an increase in cumulative pregnancy/birth rates (which wasn’t measured here).
A subgroup analysis in studies that used protocol D showed an improvement in clinical pregnancy rate when only RCTs were considered, along with studies performed in Africa.
Limitations of this meta-analysis include:
- No safety data on the use of GH for both the mother and baby.
- There was heterogeneity (variability) in the studies due to differences in ovarian stimulation protocols.
Larger RCTs are needed to address these concerns.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (4 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Meta-analysis shows growth hormone improves endometrial function
Meta-analysis shows growth hormone improves endometrial function
 Intraovarian PRP results in more eggs retrieved, but no improvement in egg quality
Intraovarian PRP results in more eggs retrieved, but no improvement in egg quality
 Study examines impact of ovarian stimulation on egg quality
Study examines impact of ovarian stimulation on egg quality
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
 Culturing immature eggs overnight by rescue IVM increases number of euploids in cycle
Culturing immature eggs overnight by rescue IVM increases number of euploids in cycle
 Early triggering with the “HIER” protocol may be a better approach for older women
Early triggering with the “HIER” protocol may be a better approach for older women
 Examining live birth rates in IVF cycles with 5 or less follicles
Examining live birth rates in IVF cycles with 5 or less follicles