
Researchers combined the results of 33 studies to evaluate how ICM, trophectoderm, and expansion grades relate to outcomes, finding that blastocysts with an A-grade trophectoderm had the strongest link to live birth, while expansion grade 2 was most associated with miscarriage.
Embryo grading is one of the main tools embryologists use to select which embryos to transfer during IVF. The most common method is the Gardner grading system, which gives each blastocyst a three-part score: the expansion stage (rated 1 to 6), the inner cell mass or ICM (graded A to C), and the trophectoderm or TE (also graded A to C). Expansion reflects how far the blastocyst has developed, the ICM develops into the fetus, and the TE develops into the placenta.
While higher grades predict better chances of success, it’s not clear how a blastocyst’s expansion, ICM or TE grade contribute. Some studies suggest the ICM grade is most important, while others find the TE grade more predictive. These differences have made it difficult to determine which part of the grading system is most useful for predicting IVF success.
This post summarizes a study by Zhang et al. (2025), who conducted a network meta-analysis of 33 studies involving nearly 70,000 embryos to assess which morphological features are most strongly associated with live birth and other IVF outcomes.
A “network” meta-analysis was used, which lets you combine studies that have different treatment protocols that aren’t directly compared. They also report the SUCRA scores (a higher SUCRA % indicates that a particular grade is better). Check the glossary for “meta-analysis” for more info.
The included studies were mainly retrospective cohort studies, published between 2007 and 2022, and had clear grading of the expansion, ICM and TE, and reported on pregnancy and neonatal outcomes.
To learn more about embryo grading, check out my post on Embryo grading and success rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Top predictors of live birth among embryo grades
Live birth outcomes were available from 19 studies, including a total of 30,651 embryos.
Here’s the results from the network meta-analysis for live birth, which directly compared the TE and ICM grades (C vs B, then B vs A), and the expansions (6 vs 5, 5 vs 4, etc.).
- TE (C) vs TE (B): -0.30 (95% CI: -0.42, -0.18) — This means that TE (C) has lower odds of live birth vs TE (B)
- TE (B) vs TE (A): -0.32 (95% CI: -0.42, -0.22) — This means that TE (B) has lower odds of live birth vs TE (A)
- ICM (C) vs ICM (B): -0.39 (95% CI: -0.58, -0.20) — This means that ICM (C) has lower odds of live birth vs ICM (B)
- ICM (B) vs ICM (A): -0.36 (95% CI: -0.46, -0.26) — This means that ICM (B) has lower odds of live birth vs ICM (A)
- Expansion (6) vs Expansion (5): -0.28 (95% CI: -0.46, -0.10) — This means that Expansion (6) has lower odds of live birth vs Expansion (5)
- Expansion (5) vs Expansion (4): 0.11 (95% CI: -0.03, 0.26) — This isn’t statistically significant, meaning that there’s no difference between Expansion (5) and Expansion (4).
- Expansion (4) vs Expansion (3): 0.20 (95% CI: 0.05, 0.36) — This means that Expansion (4) has higher odds of live birth vs Expansion (3)
- Expansion (3) vs Expansion (2): 0.15 (95% CI: -0.16, 0.46) — This isn’t statistically significant, meaning that there’s no difference between Expansion (3) and Expansion (2).
- Expansion (2) vs Expansion (1): 0.64 (95% CI: 0.16, 1.12) — This means that Expansion (2) has higher odds of live birth vs Expansion (1).
The researchers ranked embryo characteristics by their association with live birth using a SUCRA score, which ranges from 0% (least likely) to 100% (most likely).
- Trophectoderm grade A came out on top with the highest probability of predicting live birth (97.1%), followed by ICM grade A (91.1%) and expansion stage 5 (83.9%).
- Intermediate scores included expansion grade 4 (72.6%), TE grade B (59.4%), ICM grade B (44.5%), and expansion grade 6 (49.1%).
- Lower-scoring features included expansion grades 3 (43%) and 2 (27.8%), TE grade C (21.1%), ICM grade C (10%), and expansion grade 1 (0.4%).
Generally, better quality embryos with a higher expansion have a higher chance of live birth. Expansion 6 seems to have a lower chance, possibly because the embryo is more fragile.
They also did a subgroup analysis with day 5 and day 6 embryos, generally showing similar results in terms of SUCRA scoring.
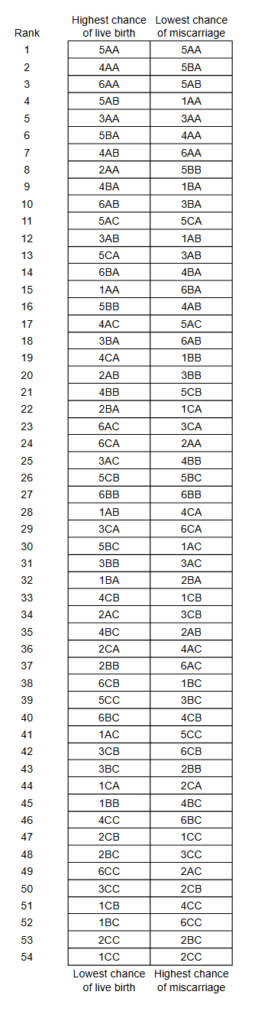
The researchers also ranked each individual embryo grade using a scoring system (by summing SUCRA scores). These rankings reflect the relative performance of each grade across all the embryo transfers.

Top predictors for miscarriage among embryo grades
Miscarriage outcomes were available from 4 studies, including a total of 6189 embryos.
The researchers ranked embryo characteristics by their association with miscarriage using a SUCRA score, where higher scores indicate a higher likelihood of miscarriage:
- The characteristics most associated with miscarriage were expansion grade 2 (86.5%), ICM grade C (82.6%), and TE grade C (81.6%).
- Intermediate scores included ICM grade B (56%), expansion grade 6 (55.2%), expansion grade 4 (52.9%), TE grade B (40.7%), expansion grade 3 (38.5%), and ICM grade A (37.5%).
- The characteristics least associated with miscarriage were expansion grade 1 (37.5%), TE grade A (17.1%), and expansion grade 5 (13.9%). This is surprising, since I would expect embryos with expansion 1 to have a higher chance of miscarriage. It’s possible this expansion wasn’t well-represented among the studies (lower sample size).
Generally, better quality embryos have a lower chance of miscarriage.
Like before, the researchers also ranked each individual embryo grade for their chance of miscarriage:

And here’s the two tables side by side if you wanted to make comparisons, but note that the scores won’t align perfectly since different studies were used to generate this data.
Conclusion
This study found that embryos with more advanced development (higher expansion stage) and higher quality grades are generally more likely to result in live birth and less likely to end in miscarriage.
There were some exceptions:
- Blastocysts with expansion 6 (fully hatched) had a lower chance of live birth. This may be because a fully hatched blastocyst is missing its zona and is more fragile. Other studies that I’ve covered haven’t found this to be the case (here and here).
- Blastocysts with expansion 1 (early blastocyst) had a lower chance of miscarriage, while expansion 2 had a higher chance of miscarriage. This might be explained by a smaller sample size, although the authors didn’t address this.
An A-grade trophectoderm showed the strongest link to live birth, with the top five embryo grades for predicting live birth being 5AA, 4AA, 6AA, 5AB, and 3AA.
Blastocysts with an expansion grade of 2 were most strongly associated with miscarriage, with the five embryo grades carrying the highest risk being 2CC, 2BC, 6CC, 4CC, and 2CB.
It’s important to note that embryo grading is very subjective and can differ from one lab to another. Even with standardized systems like Gardner, individual clinics may apply their own “house rules.” This can make grading very inconsistent between labs and between studies. This is a limitation of embryo grading in general, and by extension, is also a big limitation of this study. Advances in AI will likely make grading more standardized.
It’s also worth noting that any embryo grade, even lower-graded CC blastocysts, can still result in a healthy live birth. So please don’t let these results discourage you!
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 AI model predicts live births from blastocyst images with highest accuracy yet
AI model predicts live births from blastocyst images with highest accuracy yet
 Study examines association with embryo quality and male to female sex ratio
Study examines association with embryo quality and male to female sex ratio
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Study examines transferring a good and poor quality embryo together
Study examines transferring a good and poor quality embryo together
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 Study evaluates the potential of day 4, 5, 6 and 7 blastocysts
Study evaluates the potential of day 4, 5, 6 and 7 blastocysts