This post goes over the 2021 recommendations from the ASRM on how many embryos to transfer based on age and history of failed transfers.
Every few years the American Society for Reproductive Medicine (ASRM), publishes an updated guide for the limit of the number of embryos to transfer during IVF. This guidance is meant to optimize the chance of a pregnancy while reducing the risk of multiples.
Multiple pregnancies can be dangerous to both the mother and babies. With twins, there are increased risks of complications, including postpartum hemorrhage, chronic hypertension and organ dysfunction (maternal near miss) in the mother (Santana et al. 2016). In the child, preterm delivery, low birthweight, neonatal mortality, and long-term consequences such as cerebral palsy and learning disabilities are increased risk factors (ESHRE Capri Workshop, 2000).
So the best policy is to transfer single embryos in order to avoid these potential complications!
Clinics in the US report their outcomes to the ASRM, and if a clinic’s multiple pregnancy rate is too high, then the ASRM might audit that clinic.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
How much does transferring more than 1 embryo increase the chance of twins?
Transferring more than 1 embryo may increase the overall chance of live birth, but at the risk of multiples. The chance of a single embryo transfer splitting is about 1.56% (Ikemoto et al. 2018).
A model was prepared that predicts the chance of multiples based on age and number of embryos transferred (Awadalla et al. 2021).
For <35, with a single blastocyst transfer, the chance of a live birth is 42%. When transferring 2, it’s 58%, but 45% of those births are twins.
However, the chance of a live birth decreases with age, so more embryos are allowed to be transferred to compensate for this.
For example, from the same model, for someone who is 40 years old, a single blastocyst transfer has a predicted 17% chance of live birth. But transferring 2 has a 30% chance (15% twins), while 3 has a 40% chance (25% twins, 3% triplets).
Here’s some selected ages, and the chance of a live birth from a single blastocyst transfer vs a double blastocyst transfer (fresh) and the twin rates:
- Age 35. Single: 43% live birth; Double: 59% live birth (47% twins)
- Age 37. Single: 36% live birth; Double: 53% live birth (36% twins)
- Age 40. Single 17% live birth; Double: 30% live birth (15% twins); Triple: 40% live birth (25% twins, 3% triplets or higher)
- Age 42. Single: 5% live birth; Double: 10% live birth (4% twins); Triple: 14% live birth (8% twins)
For cleavage stage (fresh):
- Age 35. Single: 17% live birth; Double: 29% live birth (14% twins); Triple: 38% live birth (24% twins, 3% triplets or higher)
- Age 37. Single: 15% live birth; Double: 27% live birth (13% twins); Triple: 36% live birth (22% twins, 2% triplets or higher)
- Age 40. Single: 8% live birth; Double: 15% live birth (6% twins); Triple: 22% live birth (12% twins, 1% triplets or higher); Quadruple: 27% live birth (17% twins, 2% triplets or higher)
- Age 42. Single: 6% live birth; Double: 11% live birth (4% twins); Triple: 16% live birth (9% twins); Quadruple: 21% live birth (12% twins, 1% triplets or higher)
ASRM 2021 recommendations on the limits of the number of embryos to transfer
The 2021 ASRM recommendations take into account age, the stage of the embryo (cleavage stage vs blastocyst), whether or not you’re transferring a euploid embryo, and favorable prognosis criteria.
Favorable criteria can be a number of things. For instance, if this is your first frozen embryo transfer (FET), then that’s a favorable criteria because it might work the first time (or it might not – but we don’t know, so we play it safe). Women who have had a live birth from a previous transfer (using their own eggs) would also be favorable because it’s worked once already.
Favorable criteria include any one of the following (for either a fresh or frozen cycle):
- (Fresh) You expect more than 1 high quality embryo
- (Fresh) Previous live birth from transferring an embryo (from your eggs)
- (Frozen) You have frozen Day 5 or Day 6 blastocysts
- (Frozen) You have frozen euploid embryos
- (Frozen) 1st frozen transfer cycle
- (Frozen) Previous live birth from transferring an embryo (from your eggs)
So if you said “yes” to ANY of those criteria above (for either fresh or frozen), then your situation is favorable, and you need to look at that particular column in the table below.
If you said “no” to ALL of those criteria above (for either fresh or frozen), then your situation is non-favorable, and you need to look at that column below.
Euploids are always single transfers, because they have a high chance of working regardless of age.
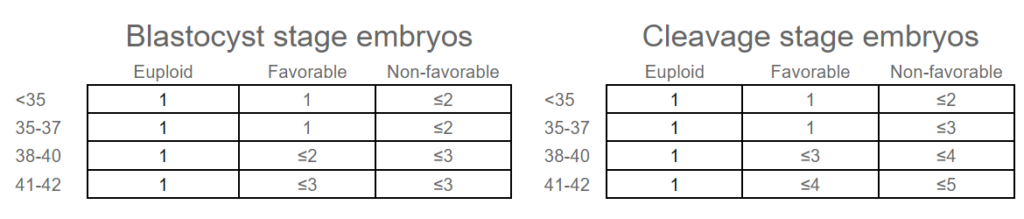
Just to be clear on what’s being shown in the table…For favorable prognosis:
- Women <38 should have a single embryo transferred.
- Women 38-40 shouldn’t have more than 3 untested cleavage stage embryos, or 2 blastocysts, transferred.
- Women 41-42 shouldn’t have more than 4 untested cleavage stage embryos, or 3 blastocysts, transferred.
If you’re favorable, but have had multiple failures after transferring high-quality embryos, an additional embryo may be considered.
Women who have pre-existing conditions (diabetes) should NOT transfer more than 1 embryo due to the further increased risks of complications with multiples.
When using donor eggs, you go by the age of the egg donor and their criteria.
For FET cycles, age/favorable criteria are set at the time the embryos were frozen. So if you were 28 when the embryos were frozen, the eggs were also 28, so you use that age. You’ll also use any favorable criteria at that time (ie. availability of frozen Day 5/6 embryos if additional embryos were frozen).
Single embryo transfers are recommended for gestational carriers (or at least following the limits as shown above based on the age of the egg donor).
For women >42 there is insufficient data for recommendations. Complications can increase with advanced age, so caution should be taken when deciding on the number to transfer.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 2 embryos or 1? The risks of a double embryo transfer for women under 35
2 embryos or 1? The risks of a double embryo transfer for women under 35
 ESHRE 2023 guidelines on the number of embryos to transfer
ESHRE 2023 guidelines on the number of embryos to transfer
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Researchers examine factors associated with preterm birth risk in IVF
Researchers examine factors associated with preterm birth risk in IVF
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles
 No differences in IVF outcomes when using fresh or frozen donor eggs
No differences in IVF outcomes when using fresh or frozen donor eggs
 Using multiple plastic consumables in the IVF lab increases risk of embryo or gamete toxicity
Using multiple plastic consumables in the IVF lab increases risk of embryo or gamete toxicity