Researchers in a 2022 study found that supplementing progesterone in true natural cycle FETs improved pregnancy outcomes.
There are several options on how to perform a frozen embryo transfer (FET), including a true natural cycle. Here, an unstimulated cycle yields a leading follicle that ovulates naturally (monitored by the LH surge), producing the corpus luteum. This produces progesterone to support the endometrium for implantation, but in many cases progesterone is supplemented exogenously (as medication) to ensure adequate levels, and it’s not clear if this is required.
For more information on this, check out my post on comparing frozen embryo transfer/FET protocols.
Wanggren et al. (2022) compared pregnancy outcomes in 243 women who received progesterone supplementation to 245 women who who didn’t using a true natural FET. This was a randomized controlled trial that took place at two centers in Sweden. Day 2, 3, 5 and 6 embryos were transferred, with both groups transferring blastocysts ~65% of the time, with no differences in quality. Nearly all were single transfers (97.5%).
Progesterone was administered as a vaginal tablet (100 mg twice a day) beginning on the day of FET until 8 weeks of pregnancy, according to their standard practice. The FET was scheduled after urinary detection of the LH surge:
- Day 2 embryos were transferred 3 days after the LH surge (LH+3)
- Day 3 embryos were transferred on LH+4
- Day 5 and 6 embryos were transferred on LH+6
This study was sponsored in part by Ferring Pharmaceuticals, which provided the vaginal progesterone tablets. However, the authors state that they had no influence over the study design, data analysis or interpretation of results.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
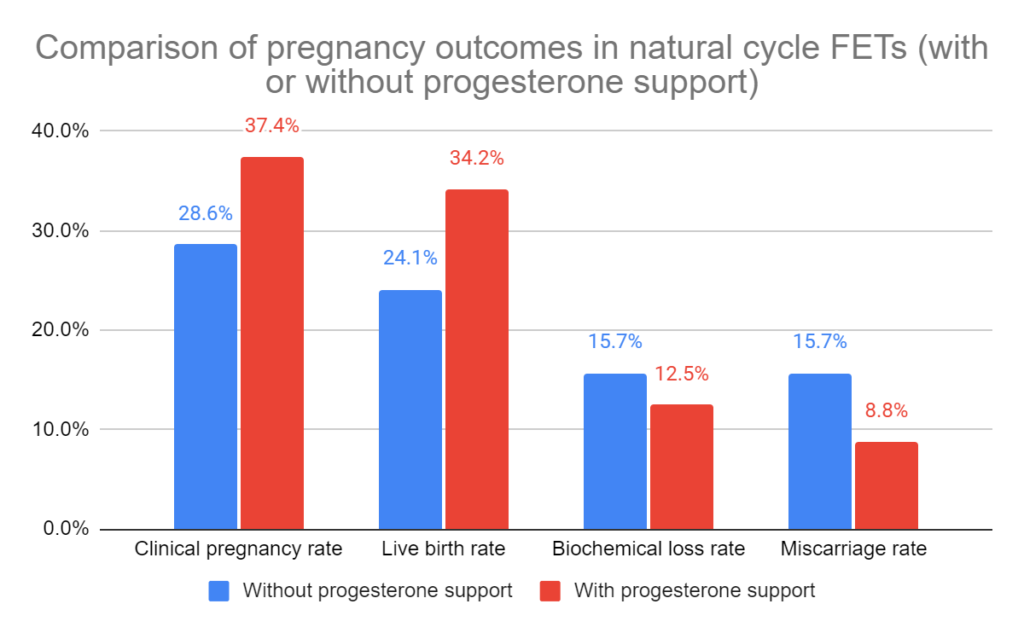
Live birth rate is improved when progesterone is supplemented
The live birth rate increased from 24.1% to 34.2% when true natural FETs had progesterone supplemented (odds ratio [95% CI]: 1.635 [1.102-2.428], p=0.017). The clinical pregnancy rate also increased. There were no statistical differences in biochemical pregnancy losses and miscarriage rates.
They also looked at outcomes after grouping cleavage stage (day 2/3) or blastocyst stage (day 5/6) transfers.
In cleavage stage transfers, the live birth rate increased from 21% to 32% with supplementation, although this wasn’t statistically significant (p=0.115). In blastocyst stage transfers, the live birth rate increased from 27% to 35% with supplementation, which was also nonsignificant (p=0.110). This may be due to the smaller sample sizes when these groups were split.
Serum progesterone levels at time of transfer had no impact on live birth rates
They measured serum progesterone levels on the day of transfer (LH+3, LH+4 or LH+6 as previously indicated). Overall, there were no differences in average serum progesterone levels in women with or without progesterone support, who did or didn’t have a live birth (roughly 11-13 ng/ml or 35-41 nmol/l).
They also compared live birth rates for women with lower progesterone levels at the time of transfer.
In this study, they used 9.1 ng/ml (29 nmol/l) as the lower threshold level for progesterone, and 3.1 ng/ml (10 nmol/l) as their extremely low threshold level. There were no statistical differences in live birth rates when comparing these thresholds, but the authors point out that this study wasn’t designed to evaluate this.

Conclusions
Overall, they found an increase in live birth rates when true natural cycle FETs were supplemented with progesterone.
This data confirms a number of studies the authors reference, except for a large retrospective study that found a decrease (Montagut et al. 2016). In this study, they supplemented progesterone one day after the LH surge (as opposed to the day of FET in this study), and the authors argue that this may have caused early closure of the implantation window.
The authors conclude that patients performing a true natural cycle FET should be offered luteal phase support with progesterone.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Live birth rates higher with natural cycle FETs vs medicated FETs
Live birth rates higher with natural cycle FETs vs medicated FETs
 Optimizing natural FET protocols: key results from a meta-analysis
Optimizing natural FET protocols: key results from a meta-analysis
 Natural FETs outperform medicated FETs in donor egg cycles
Natural FETs outperform medicated FETs in donor egg cycles
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols
 Protected sex the night before frozen embryo transfer linked to improved outcomes
Protected sex the night before frozen embryo transfer linked to improved outcomes
 How lining thickness affects success in 30,000 euploid transfers
How lining thickness affects success in 30,000 euploid transfers
 Same live birth rate, fewer complications with natural frozen embryo transfer
Same live birth rate, fewer complications with natural frozen embryo transfer
 Researchers examine how endometrial fluid before transfer affects live birth rates
Researchers examine how endometrial fluid before transfer affects live birth rates