
Sperm makes up the other half of an embryo, so naturally sperm quality is important for a successful IVF cycle. Just how important is it? In this post I’ll go over the key factors of sperm quality and address its impact on IVF success.
Note that this is an older post scheduled for an update, and may contain outdated information. For the latest information on a topic presented here, search for that topic and check out more recent posts. Thank you!
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
Defining sperm quality
Sperm represents the other 50% of your embryo, and it’s been reported that male factor infertility accounts for about 40-50% of infertility in couples, and about 7% of men overall (Kumar et al. 2015).
So when we talk about sperm quality, what do we mean?
Most of the time it’s referring to the results of a semen analysis. This is where a semen sample is collected and different parameters are measured using a microscope, including sperm concentration, motility and morphology. Other tests, like sperm DNA fragmentation, can also provide information about sperm quality.
Good quality sperm refers to sperm that:
- Can lead to successful fertilization
- Can go on to form a good quality embryo, or an embryo that is euploid
- Can lead to a pregnancy or a live birth
Essentially, good quality sperm is able to form a competent embryo that’s able to lead to a live birth. Sperm quality can be inferred by rates for fertilization, blastocyst conversion, euploidy, pregnancy, miscarriage, live birth and so on.
Of course, the egg also plays an important role in all of these factors. Having a good quality egg that can lead to successful fertilization, etc. is also important. What’s more is that the egg has DNA repair mechanisms, so in some circumstances, the egg could improve the quality of bad quality sperm.
Like egg quality, there are no specific tests that can be used to measure sperm quality reliably. There are too many factors that can cause things to go wrong with the sperm (and egg!). A lot of what can go wrong with the sperm (and egg) we can’t see with a microscope, like genetic or metabolic errors. We use the tools we can to evaluate sperm quality, like the semen analysis and DNA fragmentation tests, but these tools aren’t perfect.
Semen analysis
A semen analysis is normally performed to give an idea of the male’s fertility.
The World Health Organization releases guidance on methods to perform a semen analysis and how to interpret its quality, with their latest guidance published in 2021.
In their guidance, they include what a normal semen analysis looks like under the microscope. Below I indicate the average value followed by the 95% confidence interval in brackets (the range of normal values).
- Semen volume (ml): 1.4 (1.3–1.5). This measures the fluid volume of the semen ejaculated.
- Sperm concentration (10^6/ml): 16 (15–18). This refers to the number of sperm (in millions) present per milliliter of semen.
- Total sperm number (10^6 per ejaculate): 39 (35–40). This is the total count of sperm in the entire ejaculate, measured in millions.
- Progressive motility (%): 30 (29–31). Measures the percentage of sperm that are moving forward in a straight line or large circles.
- Non-progressive motility (%): 1 (1–1). Measures the percentage of sperm with a moving tail but move very short distances or in small circles.
- Total motility (%): 42 (40–43). This is the sum of both progressively and non-progressively motile sperm, indicating the percentage of all moving sperm in a semen sample.
- Immotile spermatozoa (%): 20 (19–20). Refers to sperm that show no tail movement.
- Vitality (%): 54 (50–56). Indicates the percentage of living sperm in a semen sample. Sperm that are moving are viable, but immotile sperm may or may not be viable. The viability of immotile sperm can be evaluated with a chemical stain.
- Normal morphology (%): 4 (3.9–4.0). Measures the percentage of sperm that have a normal shape.
This data was obtained from a study by Campbell et al. 2021, who analyzed semen samples from thousands of men in couples who achieved pregnancy within one year of unprotected sexual intercourse.
If you’re within these ranges, then your semen analysis will be considered normal. This doesn’t necessarily mean that you’re in the clear, because there could be issues that aren’t detectable with a semen analysis.
It’s a good idea to have your semen tested at least twice in close succession since there can be a lot of variability in a semen analysis and one sample often isn’t enough.
How does a semen analysis impact IVF success?
Generally, poor quality samples (low sperm concentration/motility/morphology) have reduced success (Loutradi et al. 2006):
- Fertilization drops from 77% (good sample) to 69% (poor sample)
- # of high quality day 3 embryos drops 20% to 10%
- Reduced blastocyst conversion (58% to 41%)
Another study (Borges et al. 2016) found that the most important factor was the total motile count.
Total Motile Count = (semen volume) x (sperm concentration) x (motile sperm %)
- Men with < 1 million total motile count (poorest group) had 72% fertilization
- Men with >20 million total motile count (best group) had 85% fertilization
- There were also differences in day 3 embryo grades and blastocyst formation
Sperm from poor quality semen can have more chromosomal errors (aneuploidy) than better quality samples – and this can result in more aneuploid embryos (Magli et al. 2009).
Sperm morphology
Sperm basically contain a head, midpiece and tail (highlighted below). For a sperm to be considered normal both the head and tail need to appear normal.

.
Here are some actual pictures from a microscope:
.

Remember, you only need 4% normal sperm in semen to be considered within the normal fertile range.
That means if 96% of sperm in the sample are abnormal, you’re still considered fertile!
Sperm morphology and IVF success rates
One study compared patients with or without poor morphology and found that pregnancy rates were not affected using conventional IVF or ICSI (Hotaling et al 2011).
In severe cases where only abnormal sperm are present for ICSI (De Vos et al. 2003):
- Fertilization dropped from 72% to 61%
- Day 3 embryo quality didn’t change
- The birth rate dropped from 15% to 8%
Studies have looked at sperm from fertile men and sperm from poor morphology men and found no difference in aneuploidy (Sun et al. 2006).
Severe morphologies show higher aneuploidy but these seem to be special cases.
So there isn’t a good consensus on how morphology affects IVF success rates.
Sperm DNA fragmentation (SDF)
DNA has two strands that twist around to form a “double helix” shape.
The DNA inside the sperm can sometimes be fragmented. It becomes fragmented by having “breaks” in the DNA that can occur on one or both strands. These breaks form fragments.

Breaks can occur on any chromosome, anywhere. So depending on where these breaks occur, certain genes can be damaged.
Sometimes this damage can be repaired (by the oocyte – discussed below) but if it isn’t it will be passed along to the embryo.
If the damaged gene is important, the embryo’s DNA may be impacted.
Does DNA fragmentation impact IVF success?
Yes!
In a large meta-analysis that looked at 43 studies, researchers concluded that SDF decreases pregnancy rates (Simon et al. 2017).
SDF seems to be correlated to poor semen parameters (reduced count, motility, morphology) as shown by Aydos et al. (2015) and Belloc et al. (2014).
Belloc et al. (2014) also found a subset of men who had normal semen parameters but high SDF. They speculated that these kinds of situations might account for some cases of unexplained infertility and SDF testing may be appropriate.
Although it’s a bit controversial, most evidence seems to point to no difference in embryo quality (Zini et al. 2011) or embryo aneuploidy (Gat et al. 2017).
Strange right? If the DNA in sperm is damaged, wouldn’t you expect reduced embryo quality?
The egg has a secret weapon: a DNA repair toolkit!
And this can actually fix the breaks in sperm DNA to make a healthy embryo. So fragmented sperm DNA, in the right egg, would be repaired. And in cases like this, egg quality may actually dictate sperm quality.
PESA/MESA/TESA/TESE
Some men may have trouble ejaculating sperm due to an obstruction or blockage and in cases like this sperm needs to be extracted through the epididymis (PESA or MESA) or the testicle (TESA or TESE):
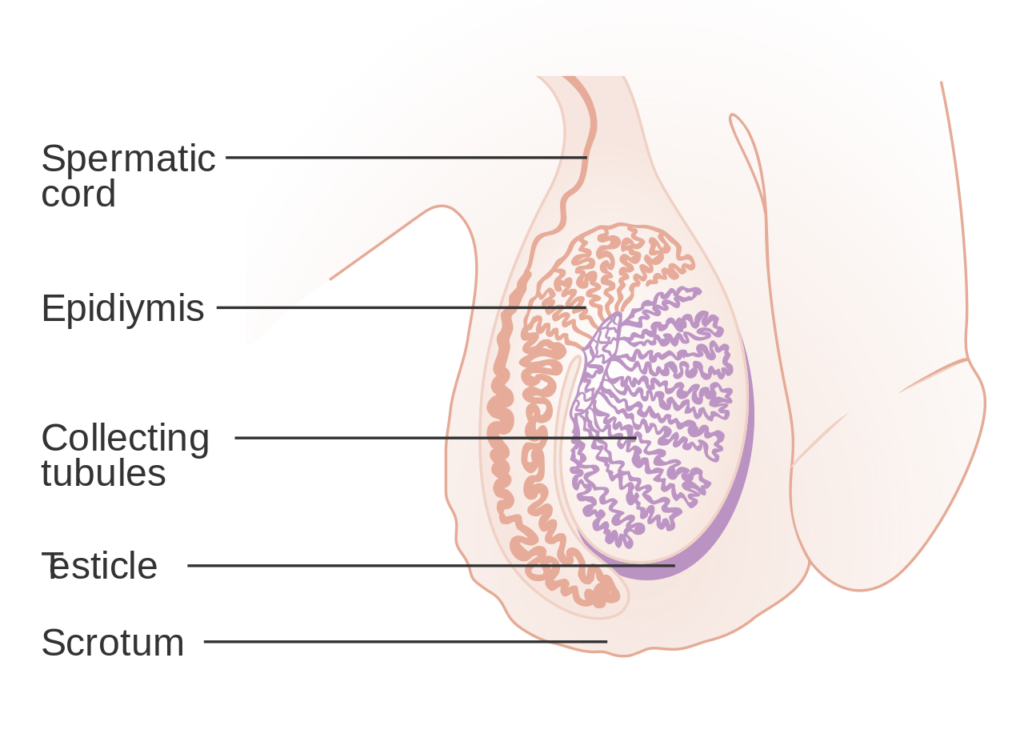
- PESA: Percutaneous Epididymal Sperm Aspiration. This is where sperm are aspirated from the epididymis using a needle
- MESA: Microsurgical Epididymal Sperm Aspiration. This is where a portion of the epididymis is dissected during an operation to aspirate sperm
- TESA: Testicular sperm aspiration. This is where a needle is used to aspirate fluid/sperm from the testicle.
- TESE: Testicular sperm extraction. This is where the testicle is biopsied and pieces are used to recover sperm.
And from these samples, motile sperm can be selected and injected by ICSI.
The performance of these non-ejaculated sperm is reviewed by Kamal et al. (2010):
- No difference in fertilization and pregnancy rates for ejaculate vs epididymal
- Another study shows lower fertilization with epididymal vs ejaculate
- Higher (or similar) miscarriage rates with testicular sperm vs ejaculate/epididymal
- No differences for fertilization and pregnancy rates in testicular vs epididymal
Advanced paternal age and sperm quality
The evidence for egg quality deteriorating with age is well established, so what about sperm?
Johnson et al. (2014) did a huge meta-analysis on 90 studies (94, 000 men) that looked at the effect on semen parameters and age:
- Semen volume, sperm count and morphology decreased slightly (small-medium effect)
- Motility and DNA fragmentation decreased about twice as much (medium effect)
- Sperm concentration didn’t change (zero effect)
This meta-analysis also showed that sperm concentrations have been decreasing globally over time (since the 1940’s!), from about 100 to 75 million/ml. This may be due to exposure to toxins and pollutants.
One study has shown that as men age, there is a decrease in embryo quality, fertilization, implantation, and pregnancy/birth rates (Johnson et al. 2014).
When young eggs (from donors) are inseminated with sperm from older men, there was no difference in fertilization or pregnancy rates (Tapia et al. 2017).
As for why sperm from older men may be compromised, it may have to do with ROS accumulation (which is typical with older age).
The composition of the sperm’s plasma membrane (the “skin” around the sperm head) makes them especially sensitive to ROS (Garrido et al. 2008) and one study has found that DNA fragmentation increases with age (Belloc et al. 2014).
Diagnosis and sperm quality
Infection
Infections can account for up to 15% of male infertility (Moretti et al. 2009), usually by impacting sperm quality. Chlamydia and gonorrhea can also impact fertility by causing scarring and creating blockages.
Bacteria, usually transmitted from intercourse, can also affect sperm quality in as many as 33% of infertile men (Moretti et al. 2009).
Treatment may involve antibiotics.
Varicoceles
Varicoceles is a condition where the veins in the testicle enlarge – kind of similar to a varicose veins in the leg. It is present in 15% of all men and 40% of men with infertility (Pathak et al. 2016).

{kind=link}
{kind=link}
{kind=link}
This may be due to blood not draining properly, resulting in enlarged veins and increased temperature, which can reduce sperm quality and increase SDF (Pathak et al. 2016).
Treatment may involve surgery.
Semen Analysis Abnormalities
Sometimes male factor infertility is identified by their Greek descriptors (Grimes et al. 2007) and relates to the WHO’s reference values for semen analysis. Here’s a list of these descriptors and their meaning:
Normozoospermia: Normal ejaculate and semen parameters
Aspermia: No ejaculate
Cryptozoospermia: Very few sperm in ejaculate (only seen after concentrating)
Azoospermia: No sperm in the ejaculate
- Obstructive azoospermia is due to a blockage
- Non-obstructive azoospermia is not related to a blockage
Oligozoospermia: Sperm concentration < 15 million/ml
Asthenozoospermia: Sperm motility < 40%
Teratozoospermia: Normal morphology < 4%
And then there’s combinations of the above that can occur:
Oligoasthenozoospermia:
- Sperm concentration < 15 million/ml
- Sperm motility < 40%
Oligoteratozoospermia:
- Sperm concentration < 15 million/ml
- Normal morphology < 4%
- Sperm motility < 40%
- Normal morphology < 4%
- Sperm concentration < 15 million/ml
- Sperm motility < 40%
- Normal morphology < 4%
Antisperm Antibodies (ASA)
Antibodies are special molecules made by the immune system that can surround and attach to a target, immobilizing it. They can act like tiny flags and alert other immune cells to destroy an infection.
Sometimes, this system can go wrong and antibodies can target our own cells – like sperm! This can impact the sperm’s performance.
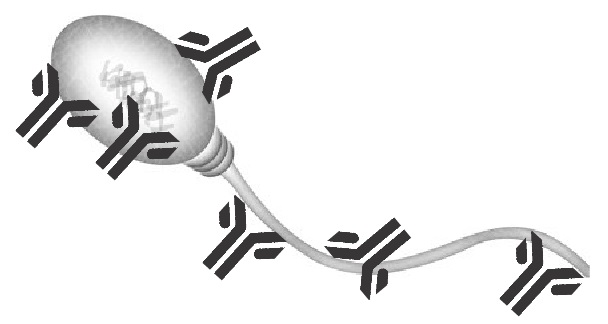
ASA occurs in about 5-15% of infertile men and can lead to reduced sperm concentration, motility, and can block sperm from binding to the zona (Cui et al. 2015).
Treatment often involves medication to suppress the immune system.
Environmental and lifestyle factors
Smoking
Firns et al (2015) summarizes the data on male smoking and sperm quality:
- Reduces semen volume, concentration, motility, and morphology
- Increases SDF
- Reduces birth rate with ICSI/conventional IVF (with a non-smoking female partner)
- Increases odds of miscarriage
Marijuana
Gundersen et al. (2015) found that regular marijuana use (more than once per week) reduced sperm concentration by 28%.
Alcohol
Firns et al. (2015) summarizes the data on alcohol consumption and sperm quality:
- Studies show a reduction in volume, concentration, motility, and morphology
- Some studies found no relationship with semen quality
- One study found an increase in fertilization
So it’s controversial! Quality is likely affected by how much/frequent people drink.
Diet
Firns et al. (2015) summarizes the data on diet and sperm quality:
- Increased consumption of fruits and vegetables improves fertilization
- Being “health conscious” (diet rich in fruits, vegetables, fish and low in meat and sugar) reduces SDF
Diets rich in soy showed a decrease in sperm concentration (Chavarro et al. 2008). This may be due to high levels of isoflavones that can disrupt hormone levels.
Heat Stress
Thonneau et al. (1998) looked at different ways high temperatures can influence fertility:
- Professional drivers (who are constantly sitting) have lower quality
- Men in wheelchairs have lower sperm motility
- Bakers, submariners, welders, and metallurgy workers all showed signs of male infertility
Men who wear briefs (instead of boxers) show reduced semen quality and increased SDF likely due to increased temperature (Sapra et al. 2015).
Improving sperm quality
ICSI/IMSI/PICSI
Sperm can have issues in binding or penetrating the zona and ICSI can be helpful in bypassing this problem by injecting the sperm directly into the egg.
There are fewer instances of fertilization failure when using ICSI vs conventional IVF and the success of both are similar (Lee et al. 2017).
Choosing normal sperm using ICSI can be challenging because abnormal sperm may not be obvious.
IMSI can overcome this by the use of a high powered microscope to select sperm that have the right stuff.
Does it work? As expected, it’s controversial (Khatun et al. 2018):
- One study showed it increased implantation 3x and pregnancy 2x
- A large meta-analysis showed no effect on pregnancy and birth rate
PICSI is another technique that can help select mature sperm by picking ones that bind to hyaluronic acid. This is the chemical on the zona that sperm naturally bind to.

Does it work? (Khatun et al. 2018):
- ICSI can help select sperm that has lower SDF
- Doesn’t improve fertilization or cleavage rate
Supplements for sperm quality
ROS and oxidative damage can be a major source in declining sperm quality (through SDF for example), so antioxidants can be important in preventing this (Ahmadi et al. 2016).
Supplementing with vitamin C and E, selenium, L-carnitine, CoQ10, zinc, and N-acetyl cysteine have all been associated with increasing semen parameters, but the data on these supplements improving embryo quality or pregnancy rates is murky.
Always discuss supplement use with your doctor before using them!
Using testicular sperm for ICSI
For men with high levels of SDF, use of testicular sperm instead of ejaculated sperm might help.
Before sperm are ejaculated, they’re stored in the epididymis and here they’re more likely to be exposed to ROS. This can lead to higher SDF in ejaculated sperm.
In the testicle, this is less of a problem.
And for men where SDF is an issue, using testicular sperm (which has lower SDF) may be beneficial (Esteves et al. 2018).

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Do sperm supplements work? Results from the MOXI trial
Do sperm supplements work? Results from the MOXI trial
 Meta-analysis confirms benefit of antioxidant supplements in infertile men
Meta-analysis confirms benefit of antioxidant supplements in infertile men
 Study reviews 34 common male fertility sperm supplement brands for safety, efficacy
Study reviews 34 common male fertility sperm supplement brands for safety, efficacy
 Paternal (male) effect on embryo aneuploidy examined
Paternal (male) effect on embryo aneuploidy examined
 Sperm aneuploidy in recurrent pregnancy loss
Sperm aneuploidy in recurrent pregnancy loss
 Evidence-based recommendations from ESHRE for 27 IVF add-ons
Evidence-based recommendations from ESHRE for 27 IVF add-ons
 Can too many supplements harm male fertility?
Can too many supplements harm male fertility?
 Endocrine disruptors and their impact on fertility
Endocrine disruptors and their impact on fertility