Researchers in a 2019 study found that an aneuploid biopsy result from the trophectoderm matched the ICM with whole chromosome aneuploidies, but not segmental aneuploidies.
One of the big questions when it comes to PGT-A/PGS testing is whether or not the 5-10 cell biopsy is really representative of the rest of the embryo (which is hundreds of cells).
Besides being aneuploid or euploid, mosaic embryos are now a well-established phenomenon, in particular with the newer NGS technology for PGT-A/PGS testing. This technology has a higher resolution and can detect smaller differences in biopsy samples. So now instead of an “aneuploid” sample we have a “60% mosaic” sample. The older PGT-A technologies, that didn’t have this level of sensitivity, might account for the contradictory results after rebiopsy.
Furthermore, the cells of the trophectoderm (where the biopsy is taken) may not match the ICM! And many are concerned that “aneuploid” embryos (as assessed by trophectoderm biopsy) may actually have euploid ICMs and be deprioritized or worse, discarded.
Victor et al. (2019) tested these questions using the superior NGS technology.
Check my complete guide to mosaic embryos to learn more about mosaics, or my complete guide to PGT-A to get more background on PGT-A (aka PGS testing).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Results
Excess embryos classified as “aneuploid” were donated to this study. Embryos were biopsied as usual, but immediately following the initial biopsy, a second biopsy of the trophectoderm (or ICM) was taken. Biopsied were subjected to NGS.
Of the 100 aneuploid blastocysts assessed by PGT-A, 93 had ICMs that were also aneuploid. So trophectoderm aneuploidy by PGT-A predicted ICM aneuploidy 93% of the time.
Most of these ICM aneuploid embryos had whole chromosome abnormalities in the trophectoderm (90/93, 96.8%), compared to segmental abnormalities (3/7, 42.9%). So trophectoderm segmental aneuploidy is less likely to predict ICM aneuploidy compared to whole chromosome trophectoderm aneuploidy.
Of the 93 embryos that had trophectoderm and ICM aneuploidy, they were divided into two groups:
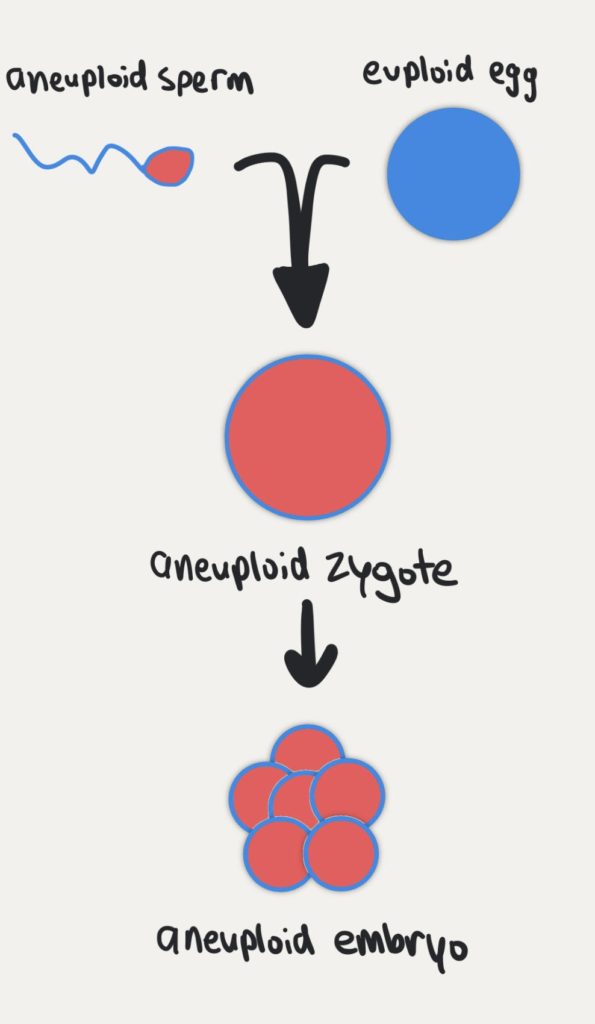
In the first group, 79 out of 93 had a perfectly matched result where the same abnormality was in both the trophectoderm and ICM. These are likely to be due to errors in the sperm or egg (ie. errors of meiosis), since every cell of the embryo is affected by the same abnormality. You can see this in the diagram below:
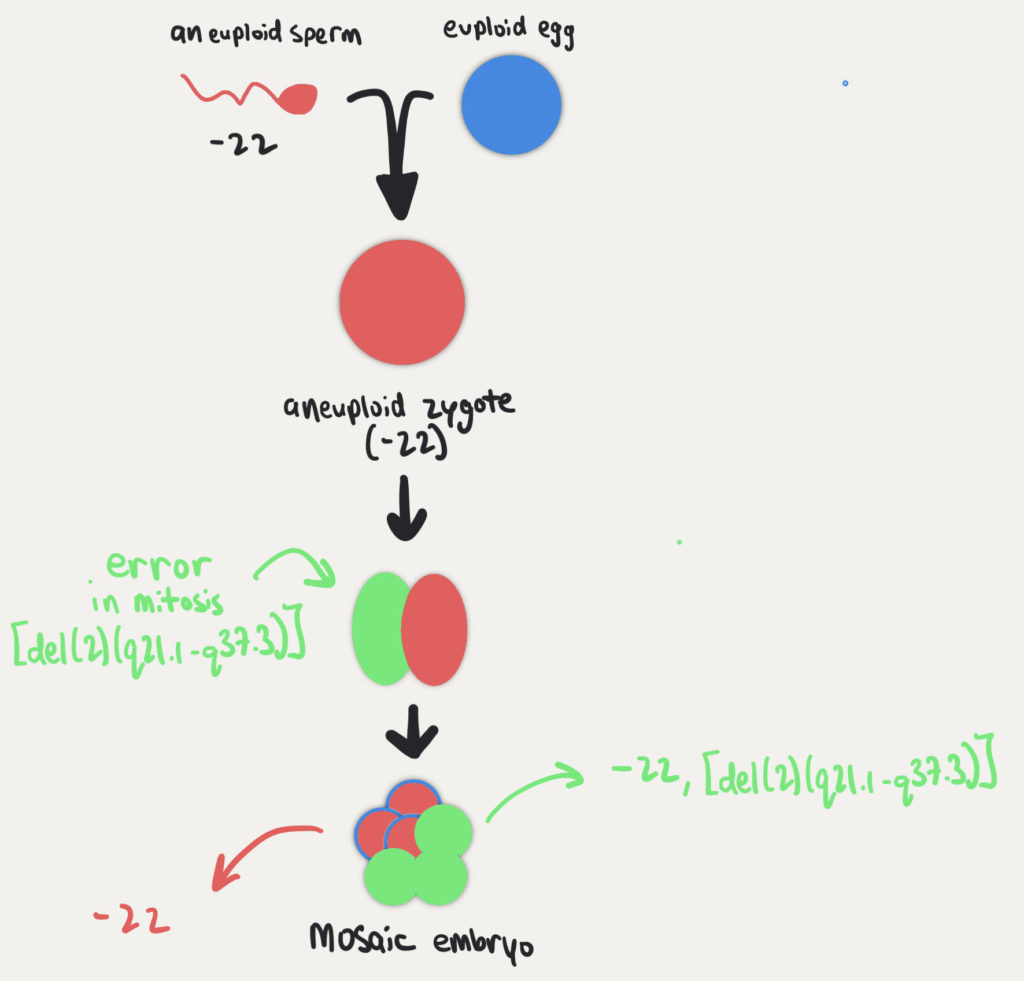
In the second group, 14 out of 93 embryos had different abnormalities in trophectoderm vs the ICM. Most of these embryos had the same initial abnormality, but an additional segmental abnormality that was mosaic in the ICM. So for example, initially it could have been -22 in the trophectoderm biopsy, but then the ICM biopsy was -22, mos[del(2)(q21.1-q37.3)] where a segmental abnormality on chromosome 2 was found in some cells of the ICM. (Read more about understanding PGT-A test results here)
This was likely due to an initial error in meiosis as shown above, followed by a error during the embryo’s cell division during mitosis to make the mosaic cells. You can see this below using the same example.
As stated above, of the 100 aneuploid blastocysts assessed by PGT-A, 93 had ICMs that were also aneuploid. As for the remaining 7 blastocysts:
- 2 had an aneuploid trophectoderm but the ICM was mosaic.
- 5 had an aneuploid trophectoderm but the ICM was euploid: 4/5 were segmental aneuploids in the first and second trophectoderm biopsy but euploid in the ICM, and 1/5 was a segmental aneuploid in the first trophectoderm biopsy but was euploid in the second trophectoderm biopsy and the ICM.
They also wanted to see if poor embryo quality had an impact on the repeatability of these biopsy results. They found that neither the blastocyst’s expansion nor the ICM or trophectoderm grade had an impact.
Conclusions
Many are critical about PGT-A/PGS testing for a number of reasons, with one common reason being the belief that a small biopsy of the trophectoderm is unlikely to be representative of the whole embryo, or of the ICM.
In this study, they found that most (96.8%) of trophectoderm biopsies predicted aneuploidy in the ICM, but only when the trophectoderm biopsy was a whole chromosome abnormality. When the trophectoderm biopsy was a segmental abnormality, this prediction dropped to 42.9%.
So why the difference between whole chromosome and segmental chromosome abnormalities?
The majority of whole chromosome abnormalities are due to errors in meiosis, where either the sperm or egg are impacted and therefore all the cells of the embryo are affected (see the graphic above). While segmental chromosome abnormalities are often due to errors in mitosis during early embryo cell division. The embryo at this stage is thought to be more careless and speedy in its initial cell divisions, and DNA breaks may be more tolerated. These types of errors are more common in mosaic embryos, where not every cell contains the same error. So mismatches in the ICM can be more common.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Does a PGT-A biopsy match the rest of the embryo?
Does a PGT-A biopsy match the rest of the embryo?
 Segmental aneuploids: the main source for PGT-A false positives?
Segmental aneuploids: the main source for PGT-A false positives?
 Mosaicism much more common than previously thought, using more sensitive PGT-A technique
Mosaicism much more common than previously thought, using more sensitive PGT-A technique
 Complete guide to PGT-A (PGS testing)
Complete guide to PGT-A (PGS testing)
 Can a mosaic embryo result in a normal baby?
Can a mosaic embryo result in a normal baby?
 Miscarriage and neonatal outcomes for over 2,000 mosaic embryo transfers
Miscarriage and neonatal outcomes for over 2,000 mosaic embryo transfers
 Multiple embryo freeze/thaw for PGT-A doesn’t affect pregnancy or neonatal outcomes
Multiple embryo freeze/thaw for PGT-A doesn’t affect pregnancy or neonatal outcomes
 A look at how PGT-A results change with age, using data from over 86,000 biopsies
A look at how PGT-A results change with age, using data from over 86,000 biopsies