Evidence up to 2022 shows that a single PGT-A biopsy is highly concordant (similar) with the rest of the embryo when the embryo is aneuploid or euploid, but not when it’s mosaic or segmental.
Looking for newer data? A 2026 meta-analysis on PGT-A biopsy mismatch rates and embryo rebiopsy is reviewed here.
A PGT-A biopsy takes only 5-10 cells from an embryo that’s potentially hundreds of cells and it’s not clear if this small sample is truly representative of the rest of the embryo. Furthermore, this biopsy is taken from the trophectoderm which develops into the placenta, and not the inner cell mass (ICM) which develops into the fetus.
Here we’ll look at three studies that compare the original PGT-A biopsy to the results of repeated biopsies to see how well they agree with each other (concordance).
Check my complete guide to mosaic embryos to learn more about mosaics, or my complete guide to PGT-A to get more background on PGT-A (aka PGS testing).
Note: One test result doesn’t overtake another, it just gives more information. A mosaic embryo is an embryo with both euploid and aneuploid cells. If the first test is aneuploid and the second is euploid, the overall result is mosaic. If the first result is mosaic and the second is euploid, the overall result is mosaic.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study 1: 2021 systematic review finds high concordance with euploid, aneuploids but low concordance with mosaics
Marin et al. (2021) did a systematic review of the available research that examined concordance of the first embryo biopsy to subsequent rebiopsies.
They found 26 studies, 17 of which involved next-generation sequencing (NGS), that were published between 2008 and 2020. Most studies rebiopsied the trophectoderm and inner cell mass (ICM), while some rebiopsied the trophectoderm, ICM or the whole blastocyst. Embryos indicated as chaotic, complex aneuploid, no result or from parents with known abnormal karyotypes were excluded.
In all, the studies included 1,124 embryos and 1,950 biopsies and comparisons:
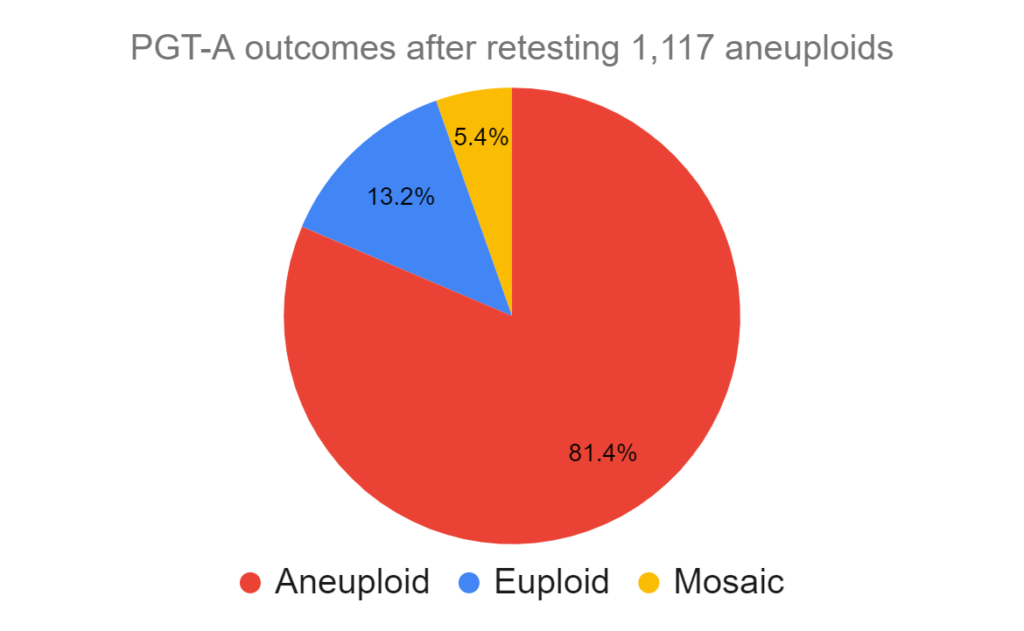
- 1,117 were initially fully aneuploid
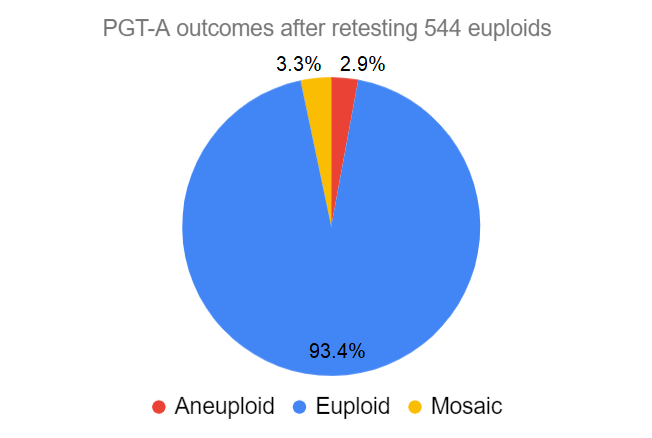
- 544 were initially fully euploid
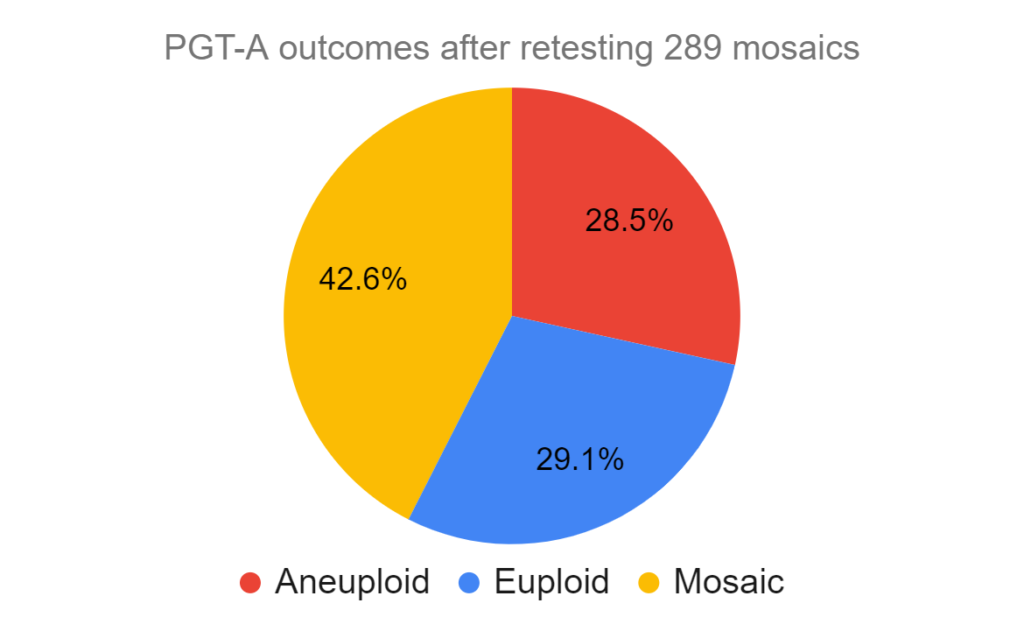
- 289 were initially mosaic
After retesting the 1,117 aneuploids, 81.4% were concordant and were aneuploid and 18.6% were nonconcordant (13.2% euploid, 5.4% mosaic).
After retesting the 544 euploids, 93.8% were concordant and were euploid, while 6.2% were nonconcordant (2.9% aneuploid, 3.3% mosaic).
After retesting the 289 mosaics, 42.6% were concordant and were mosaic, while 57.4% were nonconcordant (28.5% aneuploid, 29.1% euploid).
This study shows that there is high concordance with euploid and aneuploid embryos, but poor concordance with mosaic embryos.
Study 2: Retest of high level mosaics are mostly aneuploid, while low levels are mostly euploid
Capalbo et al. (2021) performed a randomized controlled trial (RCT) that found equivalent live birth and miscarriage rates between euploid and low/moderate level mosaic embryo transfers. I reviewed this study here if you’re interested.
In addition to this main experiment, the researchers also broke up 73 blastocysts into 5 pieces and performed PGT-A on each piece, with four pieces coming from the trophectoderm and one piece coming from the ICM. One of the trophectoderm pieces was used as the reference, and the other pieces were compared to this reference.
They compared each chromosome against the reference’s chromosome based on its result, which was categorized as:
- Euploid (if the chromosome was <20% aneuploid [aka euploid] from the reference biopsy)
- Low level mosaic (20-30%)
- Moderate level mosaic (30-50%)
- High level mosaic (50-70%)
- Aneuploid (>70%)
If you’re unclear on what these percentages mean, check out the section on PGT-A resolution in my complete guide to mosaic embryos.
They found that if the reference (first) biopsy was euploid for a particular chromosome, then there was a 99.6% chance that same chromosome would be euploid for each of the 4 additional biopsies (including the ICM). If the reference was aneuploid, there was a 98.0% chance it would be aneuploid after 4 more biopsies (including the ICM).
This shows that the concordance between euploid and aneuploid embryos is high. So if you have a euploid or aneuploid embryo and it’s rebiopsied, there’s a 98% and greater chance of the same result.
For a low level mosaic embryo, there was a 99.3% chance of the chromosome being euploid after 4 biopsies; for a moderate level mosaic there was a 95.5% chance of it being euploid; and for a high level mosaic there was a 65.0% chance of it being aneuploid.
I wanted to clarify this a little bit more with an example. Let’s say the first biopsy is 40% mosaic for trisomy 17. What these results are saying is that if you repeat the biopsy 4 more times, then there’s a 95.5% chance you’ll get a euploid result each time instead of the 40% mosaic with trisomy 17, including the ICM.
This shows that low and moderate level mosaics have a >95% chance of being fully euploid after repeat biopsies, while high level mosaics have a 65% chance of being fully aneuploid. In other words there’s a <5% chance for a low or moderate level mosaic to have the same mosaic result after 4 biopsies.
Taking this all together, this is showing that mosaicism is confined to a particular place in the embryo, and not scattered around uniformly. Euploid and aneuploid embryos, on the other hand, are uniformly euploid or aneuploid throughout the embryo.
Study 3: Euploid, aneuploid concordance is high, moderate with segmental aneuploids, low with mosaic embryos
Kim et al. (2022) performed an initial biopsy and then four rebiopsies on 300 blastocysts to determine concordance. The ICM was included but not separated (so it was mixed in with trophectoderm cells).
They used a targeted NGS platform (PGT-A-seq), which focuses on specific regions of the genome rather then the whole genome. The authors state that this has reduced technical error and improved percision compared to the more conventional whole genome amplification-based NGS platforms.
For mosaics, concordance was confirmed if there was a gain or loss on the same chromosome as the initial biopsy. For segmental mosaics, concordance was confirmed if there was any segmental abnormality on the same chromosome (mosaic or aneuploid).
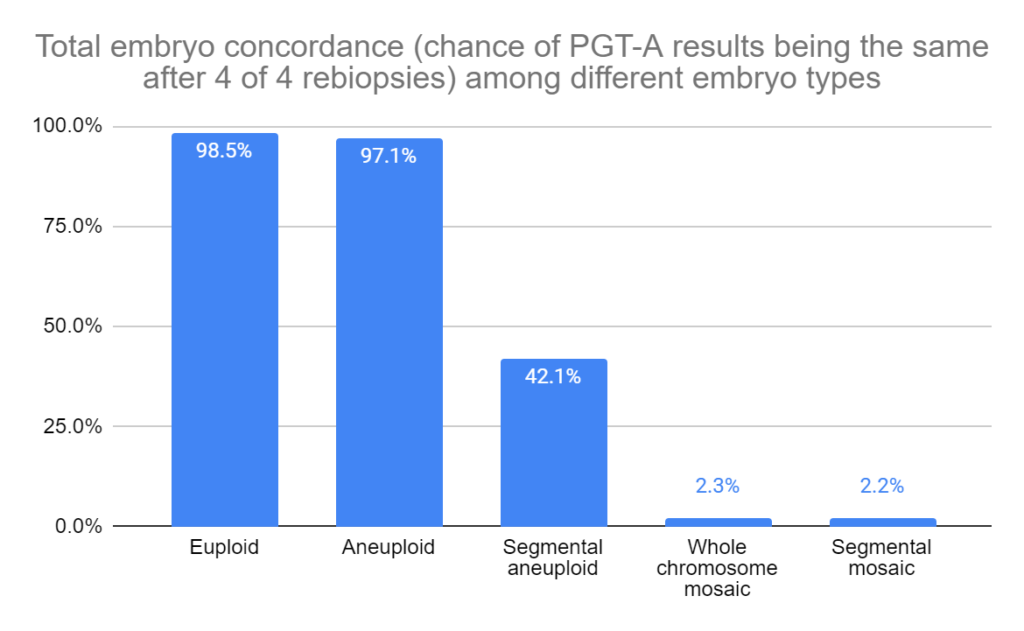
First they looked at total embryo concordance. This is where every subsequent rebiopsy matched the first biopsy.
For euploids (n=137), the total embryo concordance was 98.5%; for aneuploids (n=163), it was 97.1%; for segmental aneuploids (n=75), it was 42.1%; for whole chromosome mosaics (n=69) it was 2.3%; and for segmental mosaics (n=85) it was 2.2%.
Next they looked at partial embryo concordance rates, where at least one rebiopsy was the same as the original biopsy.
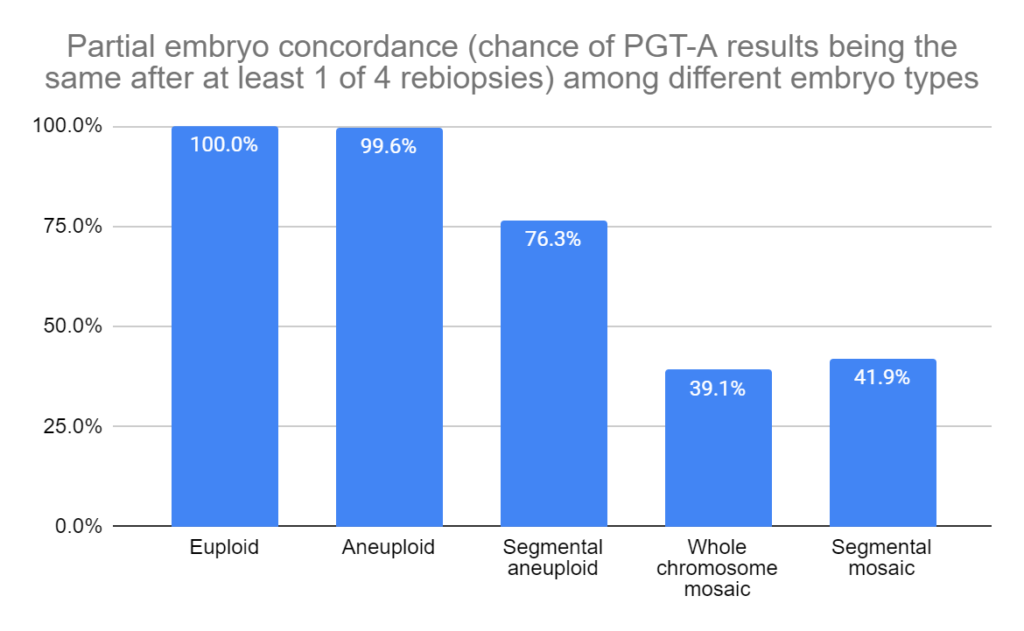
So for a whole chromosome mosaic, after doing 4 rebiopsies there was a 2.3% chance of all the rebiopsies giving the same result as the original biopsy, and a 39.1% chance of at least one of the rebiopsies giving the same result.
Overall, this study found that euploid and aneuploid biopsies were highly concordant, while whole chromosome and segmental mosaics were not. Segmental aneuploids were moderately concordant.
Like the previous study, this shows that mosaicism seems to be confined to a particular region of the embryo.
Conclusions
These studies indicate that aneuploid and euploid test results are highly concordant with the rest of the embryo, whereas mosaics are not and mosaicism seems to be restricted to a particular part of the embryo. This information doesn’t change anything in terms of clinical practice. Mosaic embryos, when transferred, still seem to have intermediate success rates to fully euploid or aneuploid embryos.
Note: One test result doesn’t overtake another, it just gives more information. A mosaic embryo is an embryo with both euploid and aneuploid cells. If the first test is aneuploid and the second is euploid, the overall result is mosaic. If the first result is mosaic and the second is euploid, the overall result is mosaic.
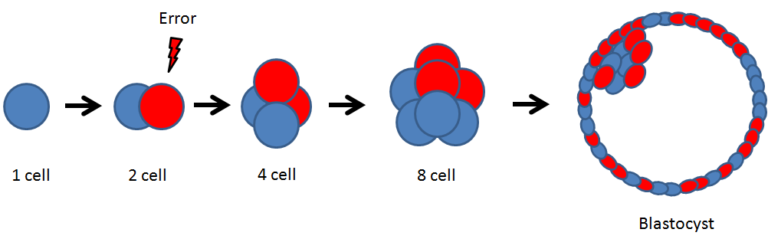
The uniformity of aneuploidy results may be because aneuploidy starts as an error in the egg or sperm (a meiotic error), which continues on from the fertilized egg to every cell in the embryo.
Mosaicism, on the other hand, comes about as errors during mitosis. This is where one cell in the embryo is affected, whereas others are not, and this aneuploid cell and its descendants are the only ones affected.
Mosaic embryos, as shown in the studies above, are not concordant with the rest of the embryo. As explained by Marin et al. (2021), there are two interpretations here:
- Nonconcordance of mosaic results is expected, since a mosaic embryo by definition contains a mix of euploid and aneuploid cells, so a retest can give different results. Based on the results above, mosaicism is confined to a particular region of the embryo and not scattered about uniformly.
- The test results are inaccurate. Treff et al. (2021) suggest that mosaic tests results are false positives, potentially due to a diagnostic error from the analysis of a suboptimal number of trophectoderm cells during a biopsy.
There is plenty of evidence that corroborates the reality of mosaic embryos besides PGT-A results (Viotti et al. 2021), although it does appear that transferring these embryos has a very low chance of actually producing a mosaic baby which is likely due to the embryo’s ability to self-correct (reviewed in my complete guide to mosaic embryos).

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Trophectoderm and ICM biopsies match depending on the abnormality
Trophectoderm and ICM biopsies match depending on the abnormality
 Complete guide to PGT-A (PGS testing)
Complete guide to PGT-A (PGS testing)
 Segmental aneuploids: the main source for PGT-A false positives?
Segmental aneuploids: the main source for PGT-A false positives?
 Can a mosaic embryo result in a normal baby?
Can a mosaic embryo result in a normal baby?
 Mosaicism much more common than previously thought, using more sensitive PGT-A technique
Mosaicism much more common than previously thought, using more sensitive PGT-A technique
 More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic
More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic
 High euploidy rates found after using PGT-A on whole embryos
High euploidy rates found after using PGT-A on whole embryos
 Real-time imaging suggests that embryo mosaicism may change over time
Real-time imaging suggests that embryo mosaicism may change over time