
Researchers in a 2023 study found that women who had a higher number of excess blastocysts frozen after their first IVF cycle had a higher live birth rate, which reached nearly 100% with 10+ excess blastocysts frozen for ages <35, 35-39 and 40+.
Beebeejaun et al. (2023) compared fresh embryo transfer outcomes among ~10,000 women who had excess blastocysts frozen after their first IVF cycle. The outcomes of 5,992 women without excess blastocysts was compared to 4,023 women with a variable number of excess blastocysts. This retrospective study took place in the UK between 2006 and 2018.
Key information:
- All cycles were first cycles and involved fresh transfer of a single day 5/6 blastocyst.
- Any excess day 5/6 blastocysts were frozen.
- Embryo quality was 3CC or higher.
- IVF or ICSI was performed.
- Women were between 20-45.
- Cycles were excluded if they involved PGT-A, egg donation, or freezing of embryos due to OHSS risk.
- The primary outcome of this study was live birth from the first fresh transfer (after 23 weeks gestation).
In terms of baseline characteristics, there were differences in the age, type of gonadotropin used, dose of FSH, number of eggs retrieved and number of eggs fertilized. Multivariate logistic regression was used to statistically adjust (control) for female age, protocol and type of gonadotropins used for ovarian stimulation, total dose of
gonadotropins administered, and number of oocytes retrieved.
Check out my complete guide to embryo grading and success rates to learn more about embryo development, grading and success rates.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Women with excess blastocysts after IVF have a higher live birth rate
Of the ~10,000 women in this study, 60% had no excess blastocysts to freeze, while 40% had 1-30 extra blastocysts (the average was 3.3). Women without extra blastocysts had on average 9.0 eggs retrieved, while those with extra blastocysts had 14.0.
Women who had one or more excess blastocysts frozen after transferring a single fresh day 5/6 embryo had a higher live birth rate compared to women without excess embryos to freeze (38% vs 24%).

After statistical adjustment to control for confounders (like age, the number of eggs retrieved, etc.), they found a 76% increase in live birth rates in women with excess embryos compared to those without (adjusted odds ratio [95% CI]: 1.76 [1.61-1.92]). This is interesting because it shows that simply making more blastocysts, independent of the number of eggs retrieved, is tied to improved live birth rates.
More embryos frozen results in a higher live birth rate across age groups
They used a “cubed polynomial regression model” to compare live birth rates for women with different numbers of excess blastocysts frozen. They did this for different age groups, including <35, 35-39 and 40 or older.
Note that this part of their study doesn’t appear to be statistically adjusted as it was above.
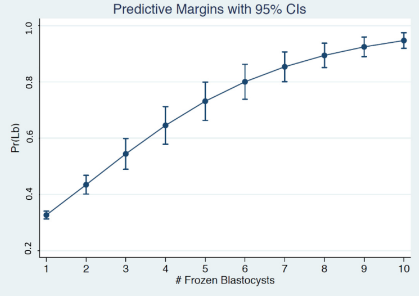
For women <35 with one excess blastocyst frozen, there was a 33% chance of live birth from the fresh transfer. This increased by 7.8% for each additional blastocyst frozen, until six (80% chance of a live birth). The model maxed out at a 95% chance of live birth when there were 10 or more excess embryos frozen.
You can see this below. The graphs show the probability of live birth on the Y axis [Pr(Lb)], with the number of excess frozen blastocysts on the X axis. The 95% confidence intervals (95% CI) are shown as bars for each point.
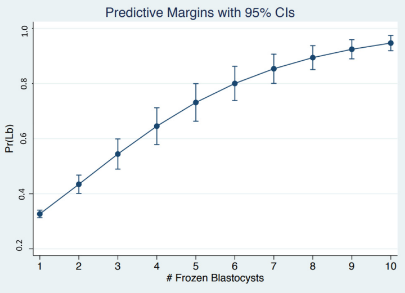
For women 35-39 with one excess blastocyst frozen, there was a 30% chance of live birth from the fresh transfer. This increased by 8.6% for each additional blastocyst frozen, until six (82% chance of a live birth). The model maxed out at a 96% chance of live birth when there were 10 or more excess embryos frozen.
For women 40 and above with one excess blastocyst frozen, there was a 26% chance of live birth from the fresh transfer. This increased by 14.3% for each additional blastocyst frozen, until four (83% chance of a live birth). The model maxed out at a 99% chance of live birth when there were 10 or more excess embryos frozen.
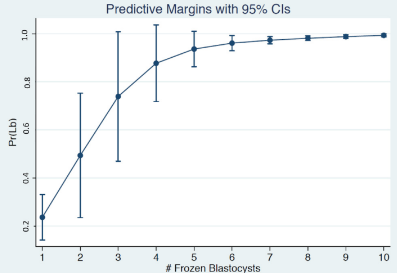
Notice the large confidence intervals in the 40 and above data. For example, the 95% CI for 1 excess blastocyst is 0.19-0.32, so the true live birth rate for 40+ women with 1 excess blastocyst (with 95% confidence) is between 19% and 32%. There’s a wider interval here because there’s a bigger difference between the live birth rate for a 40 year old and a 45 year old, compared to a smaller difference for a 35 and 39 year old. Note: It’s unclear why the 95% CIs appear to go above 1.00 in the graph, as they report the CI for 4 blastocysts is 0.68-0.97, which is below 1.00.
Conclusions
This study found that women with extra frozen blastocysts had a higher live birth rate compared to women without extra blastocysts. This was true even when controlling for the number of eggs retrieved.
This shows that the ability to produce blastocysts itself is tied to live birth rates, and women who make extra blastocysts are more likely to have success during their first transfer. Although it wasn’t discussed by the authors, this probably relates to egg/sperm quality. If the egg and sperm are able to make embryos that consistently make blastocysts, then those blastocysts may have a higher potential.
They modeled these outcomes by age (<35, 35-39 and 40+) and found that the chance of a live birth from the fresh transfer increased with each additional excess blastocyst frozen.
Women of any age with 10+ excess blastocysts had nearly a 100% chance of live birth after their first fresh transfer, while women with 1 excess blastocyst had about a 25-35% chance.
According to the authors, these findings align with previous studies on the subject, and this study represents the largest to date. They emphasize that this information can assist in doctors advising patients about their chances of success.
A limitation of this study is that they didn’t report on clinical pregnancy loss. They also grouped together day 5 and 6 blastocysts, which have been shown to have different outcomes in some studies, and they should have controlled for this.
A couple of things I wanted to address:
- First, does this apply to frozen cycles? It’s not clear, since they only looked at fresh transfers, although since some studies have found that fresh and frozen transfers have similar outcomes, it wouldn’t surprise me if they found similar results.
- Second, does this apply to second, third, etc. cycles? This study looked only looked at first cycles, so again it’s hard to say. Women with multiple cycles probably have had multiple failed transfers, so their outcomes may be different. However, this study does show that producing multiple blastocysts is tied to better outcomes for the first transfer (transfers after this would likely use lower quality embryos, so it’s not clear how they would perform). Regardless, it’s possible that a cycle that produces more blastocysts than another might have embryos with a higher potential. There may be studies that look at this, but I haven’t seen them!
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Study examines transferring a good and poor quality embryo together
Study examines transferring a good and poor quality embryo together
 Predicting how many day 3 embryos make it to blastocyst
Predicting how many day 3 embryos make it to blastocyst
 Age-specific blastocyst conversion rates and other IVF outcomes in good prognosis women
Age-specific blastocyst conversion rates and other IVF outcomes in good prognosis women
 Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation
Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success