
Researchers in a 2022 study compared IVF and pregnancy outcomes for women with low AMH (≤0.3 ng/ml) and found a decrease in live birth rates with increasing age compared to national SART rates, but these rates were comparable when low AMH women had up to 3 IVF cycles.
AMH is a marker for ovarian reserve and often predicts cycle cancellation. Typically, women with low AMH have lower success rates due to a reduced number of eggs retrieved and fewer chances of transferring embryos. A cutoff of ≤0.3 ng/ml (2.1 pmol/L) is often used for women with the lowest ovarian reserve, and it’s not clear what their chances of live birth are.
Romanski et al. (2022), in their retrospective study, compared pregnancy outcomes for 978 women with AMH levels ≤0.3 ng/ml at a single US IVF center between 2013 and 2019.
Women initiated an IVF cycle and were grouped by age:
- <35 years old (n=103)
- 35-37 (n=145)
- 38-40 (n=263)
- 41-42 (n=215)
- >42 (n=252)
As we’ll see, these “initiated cycles” will be compared with initiated cycles from US national Society for Assisted Reproductive Technology (SART) data. These women started an ovarian stimulation cycle, but because of their low AMH there were few follicles recruited and many had cancelled cycles or were converted to an intrauterine insemination (IUI) cycle.
A median of 2 cleavage stage embryos were transferred for each age group. The SART data likely includes cleavage and blastocyst stage transfers. However, including SART as a comparison is to show that women with low AMH can have live birth rates that are comparable to the national average, which is what IVF centers aim for.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Women with low AMH had a high cancellation rate and many were converted to IUI
Cancellation rates were between 19.0-26.6% for women with AMH ≤0.3 ng/ml, and between 6.8-19.4% were converted to IUI.
After considering the cancellations/conversions to IUI, the number of women who had a retrieval were:
- <35 years old (n=72)
- 35-37 (n=88)
- 38-40 (n=165)
- 41-42 (n=126)
- >42 (n=136)
The following graph illustrates this drop-off:

IVF outcomes for women with low AMH
As age increased, the median number of eggs retrieved, mature eggs, fertilized eggs and usable embryos decreased*.
*They didn’t assess if these decreases were statistically significant, so there may be no difference.

Live birth rates decreased with advanced age in women with low AMH
After accounting for the women who cancelled or had an IUI, the remaining women had a retrieval. The live birth rates decreased* as age increased.
*They didn’t assess if these decreases were statistically significant, so there may be no difference.

Per first initiated cycle, women with low AMH had lower live birth rates compared to national levels (SART)
Next, the researchers compared live birth outcomes per first initiated cycle. This is referring to all the women included in the study who initiated an ovulation stimulation cycle for IVF, even though some of them were cancelled or converted to IUI. This was done to compare to a similar statistic from SART.
Essentially, the women from the SART groups had normal AMH (as this is representing live birth rates across tens of thousands of women in the US).
There were decreases in live birth rates for each age group as shown below (statistically significant):

Comparable live birth rates to national levels when women with low AMH had up to 3 IVF cycles
Among the cohort of women with low AMH, some had an additional IVF cycle (up to 3). Below I’m indicating the original number of initiated cycles and the new number after the new cycles were started (but keep in mind this is the same group of women – there’s no new women added here, only new cycles):
- <35 years old (n=103 to 188)
- 35-37 (n=145 to 276)
- 38-40 (n=263 to 485)
- 41-42 (n=215 to 436)
- >42 (n=252 to 449)
There were additional live births with these added cycles, and this boosted the live birth rates among this group of women (cumulative rate). Compared to national SART levels, there was no statistically significant difference in live birth rates among women with low AMH (except for the <35 group).
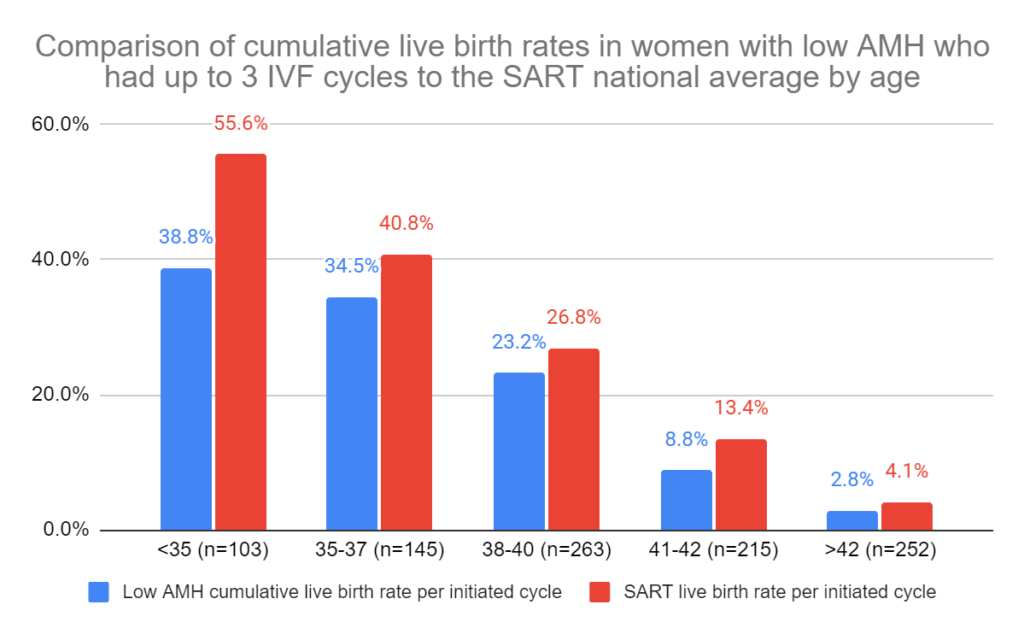
This means that women who are older than 35, had low AMH and had up to 3 IVF cycles had comparable live birth rates to national averages (with roughly normal AMH levels).
There was still a statistically significant decrease in the <35 group compared to SART. However, when they included all patients with AMH ≤0.3 ng/ml undergoing infertility treatments at their clinic there was no difference from national levels for <35 and all the other age groups. This included cumulative rates from IVF patients, ovulation induction and unassisted pregnancies.
Conclusions
This study found a decrease in live birth rates in women with AMH ≤0.3 ng/ml with advancing age.
When comparing these live birth rates to national SART levels (with average AMH levels), there was a statistically significant decrease for each age group. However, when low AMH women had up to 3 IVF cycles, there was no longer a difference to national levels, except for women <35. This shows that most women with low AMH can have live birth rates that are comparable to national levels when they have up to 3 IVF cycles.
Even though there was a decrease in the <35 group, this group still had acceptable live birth rates but they weren’t as high as the national level.
However, when the researchers included live birth outcomes from all infertility patients at their center, and not just IVF patients, this boosted the live birth rate for all age groups and there were no differences from national levels.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Accelerated biological age linked to lower AMH, number of eggs retrieved
Accelerated biological age linked to lower AMH, number of eggs retrieved
 Study finds poor ovarian responders have no further live births after 4 cycles
Study finds poor ovarian responders have no further live births after 4 cycles
 Comparing IVF outcomes from cycles with low AMH
Comparing IVF outcomes from cycles with low AMH
 Factors impacting success in second IVF cycles: age, protocol changes and more
Factors impacting success in second IVF cycles: age, protocol changes and more
 AMH levels by age and how it relates to diminished ovarian reserve (DOR)
AMH levels by age and how it relates to diminished ovarian reserve (DOR)
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles
 Impact of delayed treatment on IVF outcomes
Impact of delayed treatment on IVF outcomes
 Examining live birth rates in IVF cycles with 5 or less follicles
Examining live birth rates in IVF cycles with 5 or less follicles