Researchers in a 2024 study found lower cumulative live birth rates in patients with a particular type of endometriosis (DIE and/or ovarian endometrioma) that was diagnosed using transvaginal ultrasound.
There are different types of endometriosis, and this study wanted to compare live birth rates in women with or without deep infiltrating endometriosis (DIE) and/or ovarian endometrioma, who were diagnosed using transvaginal ultrasound.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including the number of patients and their characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a prospective cohort study that took place at an IVF center in Sweden between 2018 and 2021.
- All women were having their first IVF cycle, and had a transvaginal ultrasound to diagnose endometriosis before treatment started.
- The ultrasound technician was specialized in detecting endometriosis.
- Ovarian endometrioma and DIE were evaluated using guidelines from the International Deep Endometriosis Analysis (IDEA) group.
- A single cleavage stage or blastocyst stage embryo was transferred fresh, unless there were risks of OHSS. Excess blastocysts were frozen for an FET.
- The primary outcome was cumulative live birth rate, after fresh and frozen transfers from the first cycle (but not all embryos were necessarily used).
In terms of sample size, there were 1,040 women in the study:
- 234 with endometrioma and/or DIE (115 had endometrioma; 185 had DIE; 49 had endometrioma without DIE; 119 had DIE without endometrioma)
- 806 without endometrioma/DIE
In terms of patient characteristics, the average age was 32 and there were differences in AMH levels, type of ovarian stimulation protocol, FSH dose, use of ICSI/IVF, and embryo transfer day. These differences were statistically adjusted for in their analysis.
Note that there were many differences in patient characteristics because the patients received individualized treatments depending on their AMH levels and endometriosis, and their preferences.
Women with DIE and/or endometrioma have a reduced cumulative live birth rate
Overall, women with DIE and/or endometrioma had a lower cumulative live birth rate vs women without the diagnosis (33.3% vs 43.2%; adjusted relative risk [95% CI]: 0.63 [0.48-0.82]).
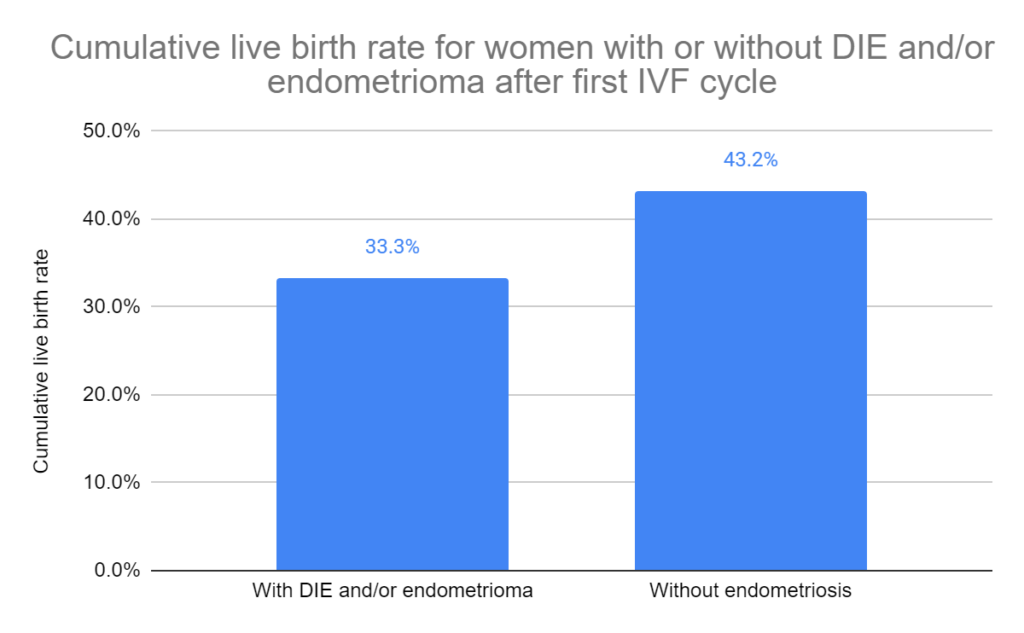
This cumulative rate includes both fresh and frozen transfers, and as we’ll see in the next section, this decrease is due to a decrease in live births from fresh transfers, not frozen transfers.
Women with endometrioma (and no DIE) had a lower cumulative live birth rate vs patients without it (24.5% vs 43.2%, p= 0.010). Women with DIE (and no endometrioma) had similar rates vs those without it (37.0% vs 43.2%, p= 0.201).
They also looked at cumulative pregnancy loss rates, and found no differences.
A look at fresh or frozen transfers in patients with DIE and/or endometrioma
The data above was for the cumulative live birth rates — including both fresh and frozen transfers from a single IVF cycle.
So what does the data look like when we look at only fresh or frozen transfers?
For fresh transfers, the live birth rate was lower for patients with DIE and/or endometrioma vs those without (29.0% vs 41.8%; adjusted relative risk [95% CI]: 0.61 [0.44-0.84]). For the sample size, there were 588 fresh transfers in women without endometriosis and 176 with DIE and/or endometrioma.
For frozen transfers, the live birth rate was similar (28.1% vs 33.3%). For the sample size, there were 306 FETs in women without endometriosis and 96 FETs in women with DIE and/or endometrioma.
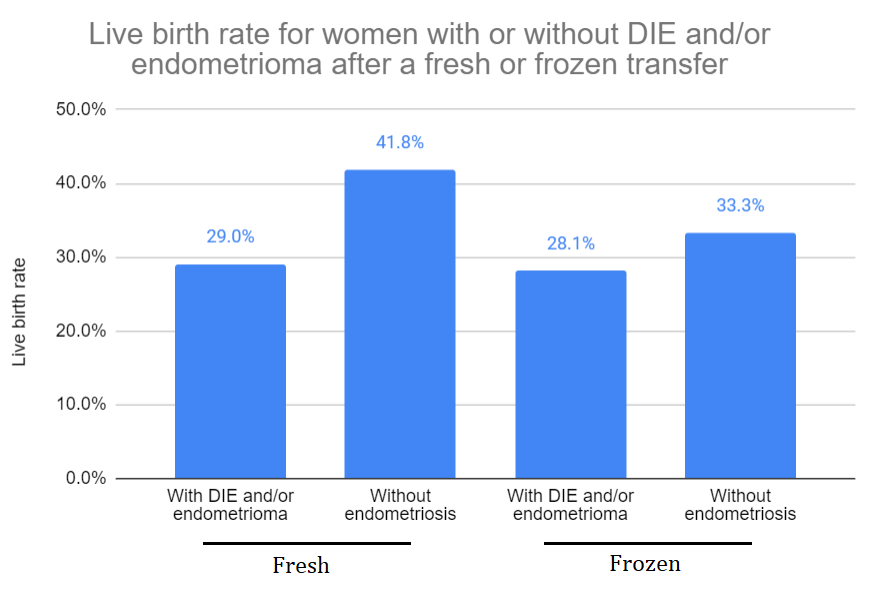
This shows that a fresh transfer results in a lowered live birth rate in DIE/endometrioma patients, so this is why the cumulative rate above was decreased.
There’s a couple of potential reasons for this:
- There were more women who did a fresh cleavage stage transfer in the endometrioma and/or DIE group vs the control group (59.7% vs 50.3%, p= 0.021), and cleavage stage embryos may have a lower success rate than blastocysts. In the frozen group, they were all blastocyst transfers. Note: I think they could have statistically adjusted for cleavage vs blastocyst stage transfers here to see if there was still a difference, but as far as I can tell they didn’t.
- Evidence is emerging that shows that fresh transfers decrease live birth rates for patients with endometriosis compared to frozen transfers. This is because endometriosis is an estrogen-dependent condition, and the high levels of estrogen present during a fresh transfer (after ovarian stimulation) can exacerbate endometriosis and potentially lead to reduced endometrial receptivity.
They also looked at pregnancy loss rates, and found no differences.
Embryology outcomes for patients with DIE and/or endometrioma
They also compared embryology outcomes for the groups. For patients without endometriosis vs those with DIE and/or endometrioma, there was:
- No difference in cancelled egg retrieval cycles (2.2% vs 2.1%).
- No difference in number of mature eggs retrieved (9 vs 8).
- No difference in fertilization rate (53% vs 52%).
- No difference in total fertilization failure (6.3% vs 9.4%).
- No difference in the number of good quality embryos (1 vs 1).
- No difference in the % of cycles with good quality embryos (79.2% 79.9%).
Conclusions
This study found that women with DIE and/or endometrioma had a lower cumulative live birth rate than patients without endometriosis.
When they looked at fresh and frozen transfers separately, they found that patients with fresh transfers had a lower live birth rate, but not patients who did a frozen transfer. This could be due to a higher number of cleavage stage embryo transfers in the fresh group, or differences in how endometriosis patients respond to fresh vs frozen transfers.
There were no differences in embryology outcomes, like the number of mature eggs retrieved or fertilization rate.
They also found that patients with endometrioma alone had a lower cumulative live birth rate than women with DIE alone. Some DIE lesions in this study were small, and larger endometrioma may produce more inflammation that might reduce success. However, the study wasn’t powered to draw conclusions from these smaller groups.
There have been mixed results in studies that compare IVF success rates in patients with or without endometriosis (referenced below). The authors believe this is partly due to differences in study design and protocols used:
- Differences in how endometriosis is diagnosed (laparoscopy, pelvic examination, ultrasound — possibly without clear diagnostic criteria)
- Diagnosis with laparoscopy often uses the ASRM’s classification, which doesn’t include DIE.
- Some studies surgically treat endometriosis while others don’t.
- Some studies rely on a self-diagnosis of endometriosis.
- Some studies might underdiagnose endometriosis. Many patients who have endometriosis may not have symptoms (silent endometriosis).
- Emerging evidence is showing that there may be differences between fresh and frozen transfers in patients with endometriosis. Some studies might only transfer fresh, or frozen.
A limitation of this study is that the patients weren’t examined by laparoscopy, although the authors assert that the IDEA method by ultrasound has been shown to have good diagnostic accuracy compared to laparoscopy for endometriosis. They also acknowledge that not all ultrasound technicians may be trained to detect endometriosis, so the results might not be generalizable.
Related studies
There were a number of studies referenced that you might want to check out, as shown below (10 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Adenomyosis by MRI reduces live births in endometriosis patients
Adenomyosis by MRI reduces live births in endometriosis patients
 Meta-analysis compares impact of endometriosis on IVF, obstetric and perinatal outcomes
Meta-analysis compares impact of endometriosis on IVF, obstetric and perinatal outcomes
 Researchers develop tool to predict pregnancy after IVF for endometriosis patients
Researchers develop tool to predict pregnancy after IVF for endometriosis patients
 Explaining unexplained infertility through non-surgical endometriosis diagnosis
Explaining unexplained infertility through non-surgical endometriosis diagnosis
 Patients with or without endometriosis have similar live birth rates after PGT-A
Patients with or without endometriosis have similar live birth rates after PGT-A
 Nearly half of unexplained infertility patients have endometriosis
Nearly half of unexplained infertility patients have endometriosis
 Meta-Analysis looks at hormone pre-treatment (Lupron Depot) for IVF with endometriosis
Meta-Analysis looks at hormone pre-treatment (Lupron Depot) for IVF with endometriosis
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles