Researchers in a 2026 randomized controlled trial found that natural FETs using euploid embryos led to lower early pregnancy loss rates and higher live birth rates than medicated transfers, although the study was stopped early.
Frozen embryo transfer (FET) cycles can be performed using either a natural cycle, where ovulation occurs naturally, or a medicated cycle, where estrogen and progesterone are given to prepare the endometrium. Medicated cycles are often easier to schedule, but some studies have suggested they may be associated with higher rates of pregnancy complications and pregnancy loss.
One challenge when studying pregnancy loss is that many miscarriages are caused by chromosomal abnormalities in the embryo. This makes it harder to know if any differences in FET success rates are due to the embryo itself or the endometrial environment.
To address this, Roelens et al. (2026) conducted a randomized controlled trial using euploid embryos for both natural and medicated FETs to see whether there was any difference in early pregnancy loss. By using euploid embryos, they could better isolate the effect of the FET protocol itself.
For more background, check out my post Comparing frozen embryo transfer/FET protocols.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: Randomized controlled trial conducted between 2019 and 2024 at a university fertility center in Belgium
- Participants: 354 women (average age about 32) undergoing their first FET of a single euploid blastocyst after PGT-A (13.6%), PGT-M (68.1%), or PGT-SR (18.4%). Notably, most participants underwent PGT-M to avoid passing on a genetic condition rather than for infertility itself. All patients had regular menstrual cycles.
- Natural FET (n= 178). These were true natural FETs, without an hCG trigger.
- Medicated FET (n= 176)
- 354 patients were in the intention to treat analysis, with 328 completing the study per protocol (natural FET: 169 and medicated FET: 159)
- Embryos: Single euploid blastocyst transfer. The study initially included only top- and good-quality day 5/6 blastocysts, but eligibility was expanded in 2023 to include some lower-quality and day 7 embryos.
- Primary outcome: Early pregnancy loss before 8 weeks gestation
- Trial registration: NCT03976544
Lower early pregnancy loss with natural FET
The primary outcome of this study was early pregnancy loss (before 8 weeks) after a single euploid transfer for natural vs medicated FET. They found that natural FETs resulted in a lower early pregnancy loss compared to medicated FETs (6.7% vs 14.2%, risk difference [95% CI]: -7.5 [-13.8 to -1.1], p= 0.022)
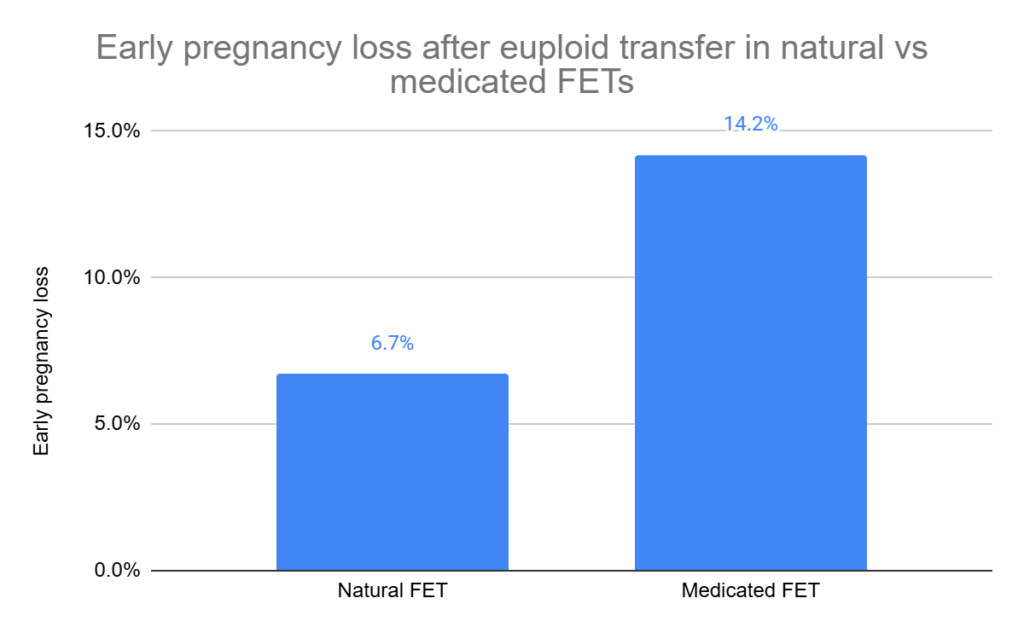
This was in the intention to treat (ITT) analysis. The per protocol (PP) analysis also showed a significant difference (7.1% vs 15.7%).
They also found large differences in the live birth rate for natural vs medicated FET (67.4% vs 47.2%, risk difference [95% CI]: 20.3 [10.2 to 30.3], p< 0.001). Similar results were also seen in the PP analysis (70.4% vs 52.2%).
No change in pregnancy complications or birth outcomes
The researchers didn’t find statistically significant differences in:
- Gestational age at delivery
- Birth weight
- Mode of delivery
- Hypertensive disorders of pregnancy (like preeclampsia)
However, the study was not powered to detect differences in these outcomes, so smaller effects could have been missed.
Conclusion
In this randomized trial, natural FETs were linked to lower rates of early pregnancy loss and higher rates of live birth compared to medicated FETs. This suggests that the way the endometrium is prepared may affect implantation and early pregnancy development, even when the embryos are chromosomally normal.
One possible explanation is the presence of the corpus luteum in natural cycles. In addition to producing progesterone, the corpus luteum releases other hormones and signaling molecules that could help support implantation, placental development, and a healthy pregnancy. Because medicated FETs don’t include a corpus luteum, this might explain some of the differences between the groups. However, the researchers didn’t find any differences in hypertensive disorders of pregnancy (like preeclampsia), although the study wasn’t powered to detect these differences.
Although live birth was significantly higher in the natural FET group (67.4% vs 47.2%), the confidence interval was fairly wide (10.2% to 30.3%), suggesting some uncertainty about the true size of the benefit. Because the study was designed around early pregnancy loss rather than live birth, this finding should be interpreted cautiously until confirmed in other studies.
Other studies have been mixed on this topic, with some reporting an improvement in miscarriage rates and others finding no difference. A recent Cochrane review by Ghobara et al. (2025) found no clear difference, although the analysis was based largely on a single randomized trial and only included evidence available up to 2022, before the more recent studies that reported improvements were available. For pregnancy complications, a recent meta-analysis reported lower rates of hypertensive disorders of pregnancy with natural FETs.
Overall, these findings add to the growing evidence that natural FETs may lead to better pregnancy outcomes than medicated FETs in patients who ovulate regularly. However, the overall evidence is still mixed, and additional randomized trials are needed before firm conclusions can be made.
Limitations:
- Most patients used PGT-M. About 68% of participants used PGT-M to avoid passing on a genetic condition rather than for infertility itself. These patients may differ from the broader IVF population, so the results might not apply to all IVF patients.
- The study was stopped early. The researchers planned to enroll 522 patients but stopped the trial after enrolling 354 due to concerns from other studies about possible pregnancy complication risks with medicated FETs. While the primary outcome was statistically significant, the confidence interval was fairly wide (-13.8% to -1.1%), suggesting some uncertainty about the true size of the effect.
- Embryo characteristics were not fully reported and changed during the study. The distribution of day 5 and day 6 blastocysts was not reported, and in 2023 the eligibility criteria were expanded to include some lower quality embryos and day 7 blastocysts. The authors didn’t report if this was balanced between the groups, even though embryo stage and quality can affect IVF outcomes.
Want to read more about hCG and pregnancy outcomes after IVF?
Researchers in a 2026 study found that natural FETs using donor eggs were linked to higher live birth rates, lower miscarriage rates, and lower rates of some pregnancy complications compared to medicated FETs. Read more.

Researchers in a 2023 study found decreased adverse pregnancy and neonatal outcomes in those who performed a natural vs medicated FET, including abnormal birth weights, preeclampsia, preterm births, and more. Read more.

A 2025 randomized controlled trial found that natural cycle FETs led to higher live birth rates and fewer miscarriages than medicated FETs in ovulatory women with a good prognosis. Read more.
A 2026 randomized trial found that natural FETs had similar healthy live birth rates to medicated FETs, but were linked to lower risks of preeclampsia, pregnancy loss, and some other pregnancy complications. Read more.
Reference
C Roelens, S Santos-Ribeiro, S Mackens, A De Vos, K Keymolen, P Verdyck, M De Vos, H Tournaye, W Verpoest, C Blockeel, The impact of endometrial preparation on pregnancy loss in vitrified-warmed euploid blastocyst transfer cycles: a randomized controlled trial, Human Reproduction, Volume 41, Issue 6, June 2026, Pages 910–917, https://doi.org/10.1093/humrep/deag060

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.