A 2024 study found that patients with recurrent pregnancy loss have congenital uterine anomalies at a rate of 8-19%, with 23% having adenomyosis.
Recurrent pregnancy loss (RPL) is the loss of two or more pregnancies and affects between 1-4% of all women (Dimitriadris et al. 2020). Uterine anomalies are irregularities in the structure of the uterus that could lead to RPL.
The study reviewed here by Busnelli et al. (2024) uses 2D and 3D ultrasound to diagnose uterine anomalies in women with RPL to see how prevalent they were. Note that this study is simply reporting on the prevalence of these anomalies in RPL patients, and isn’t comparing them to non-RPL patients.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- This was a retrospective cohort study by Busnelli et al. (2024) conducted between two university hospitals in Italy between 2020 and 2023.
- Women had RPL, defined as having two or more pregnancy losses in the first trimester. They were also between 25-42 years old, were not infertile and never had IVF or an IUI.
- Women with RPL had both a 2D/3D ultrasound during the luteal phase to diagnose uterine anomalies.
In terms of sample size, there were 442 women in this study.
Congenital anomalies found in 8-19% of women with recurrent pregnancy loss
This study used 2D and 3D transvaginal ultrasound to diagnose different uterine anomalies. These anomalies can be classified by different systems, such as ESHRE/ESGE, ASRM or CUME. In this summary I’ll just be including ESHRE/ESGE’s and the ASRM’s classification.
The European Society of Human Reproduction and Embryology (ESHRE) and the European
Society for Gynaecological Endoscopy (ESGE) established a common classification system for congenital uterine anomalies in 2013 (Grimbizis et al. 2013).
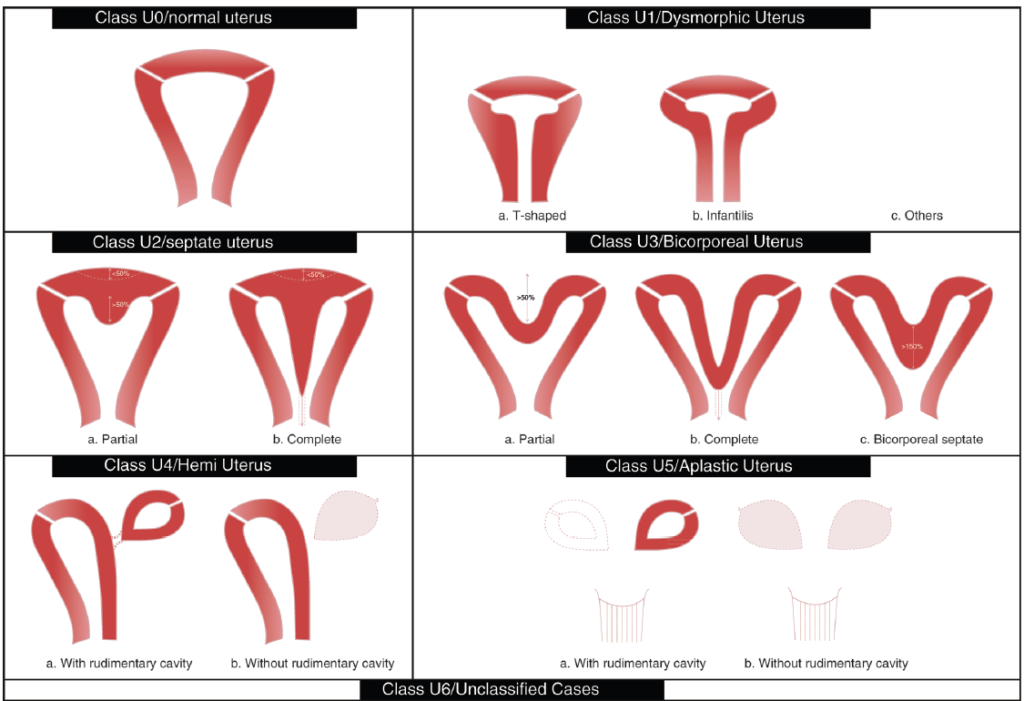
The ASRM has a similar system that is more simplified compared to ESHRE/ESGE, and classifies the same types of anomalies with differences in their phrasing and definitions (Pfeifer et al. 2021). A “bicornuate” uterus with ASRM is “bicorporal” with ESHRE/ESGE (Class U3); a “unicornuate” uterus with ASRM is a Class U4b with ESHRE/ESGE (aka a hemi uterus without a rudimentary cavity).
You can see how common these anomalies were below, with the ESHRE/ESGE classification on the left and the ASRM classification on the right. The most common anomaly was the Class U1c (other) at 18%, followed by Class U2a (partial septate uterus) at 14% by ESHRE/ESGE. Using ASRM’s classification, there were only 7% of women with a partial septate uterus, due to differences in how these anomalies are defined.

In total, the authors note that congenital anomalies were found in 19% of women by the ESHRE/ESGE system (when excluding Class U1c or others) and 8% by the ASRM system. Note that you get these percentages when you add the up numbers; the percentages above are rounded so when you add them up they’re higher than 19% or 8%.
Nearly a quarter of RPL patients had adenomyosis
Besides the congenital anomalies that were detected by 2D and 3D ultrasound, the researchers also found that a high proportion of RPL patients had adenomyosis (23%).
RPL women who never gave birth had a higher rate of adenomyosis compared to RPL women who had given birth (27% vs 11%, p< 0.001). Adenomyosis was also more common in women who had three or more pregnancy losses compared to those with two losses (29% vs 15%, p< 0.001). This suggests that adenomyosis might lead to more severe RPL.
There were no differences in the prevalence of congenital uterine anomalies based on birth history or number of pregnancy losses.
They also reported on polyps and fibroids:
- Endometrial polyps: 4% of women.
- FIGO 0-3 fibroids: 4%.
- FIGO 3-5 fibroids: 16%.
- FIGO 6-7 fibroids: 8%.
- FIGO 3-5 fibroids that are larger than 4 cm: 3%.
Conclusion
Congenital uterine anomalies were detected in 8-19% of RPL patients (depending on the classification system used). A partial septate uterus was diagnosed in 7-14% of patients, while a T-shaped uterus was diagnosed in 4% of patients using the ESHRE/ESGE system.
Nearly a quarter of RPL patients had adenomyosis, which was more common in women who never had a birth, or in those who had three or more pregnancy losses. Adenomyosis has been associated with miscarriage (Cozzolino et al. 2022) and it’s possible that adenomyosis can lead to more severe RPL, but further studies are needed.
Endometrial polyps were diagnosed in 4% of women, and fibroids were found in 4-16% of women (depending on their classification).
In general, other studies that report on congenital uterine anomalies, adenomyosis and fibroids have variable data. The authors note that this is because of differences in diagnostics (hysteroscopy, 2D or 3D ultrasound) and the system of classification used:
- Congenital anomalies (excluding arcuate uteruses) are found in 3-15% of RPL patients (Bohlman et al. 2010, Chan et al. 2011, Sugiura-Ogasawara et al. 2013, Youssef et al. 2020). The Chan et al. 2011 study was an older review that included 94 studies, finding that uterine anomalies were present in 5.5% of the unselected population, 8.0% in infertile women, 13.3% in those with a history of miscarriage and 24.5% in those with miscarriage and infertility.
- Adenomyosis is found in 12-38% of RPL patients (McCormack et al. 2016, Puente et al. 2016, Atabekoğlu et al. 2020). The Puente et al. 2016 study found that adenomyosis was more common in patients with RPL vs those without it (38.2% vs 22.3%).
- Fibroids are found in 8-15% of RPL patients (Bohlman et al. 2010, McCormack et al. 2016, Puente et al. 2016)
So does having surgery to correct these anomalies benefit patients? The study reviewed here indicated a couple of studies that related to septum resection (in septate uteruses).
- A recent trial found no improvements in live birth after hysteroscopic septum resection (Rikken et al. 2021).
- A meta-analysis that included retrospective/prospective studies found that septum resection reduced the risk of miscarriage, leading the authors to recommend resection in cases of pregnancy loss (Carrera et al. 2022).
Based on their data and previous data, the authors recommend that patients with two pregnancy losses should consider a 3D ultrasound to help diagnose uterine anomalies.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Meta-analysis examines impact of small fibroids on pregnancy outcomes
Meta-analysis examines impact of small fibroids on pregnancy outcomes
 Whole exome sequencing used to identify 6 genes involved in recurrent euploid miscarriage
Whole exome sequencing used to identify 6 genes involved in recurrent euploid miscarriage
 Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes
Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes
 Increases in immune cells associated with reduced risk of miscarriage
Increases in immune cells associated with reduced risk of miscarriage
 The role of the immune system in infertility and IVF
The role of the immune system in infertility and IVF
 Small genetic mutations in euploid pregnancies linked to miscarriage
Small genetic mutations in euploid pregnancies linked to miscarriage