
Successful embryo implantation and pregnancy depends on careful control of the immune system. In this post, we’ll explore the general workings of the immune system and its role in pregnancy, examining how dysregulation of immune cells like natural killer (NK) cells and macrophages can impact fertility. Additionally, we’ll look into autoimmunity and discuss how immunotherapies may be used to improve IVF outcomes.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
How the immune system works
The immune system is the body’s defense mechanism against pathogens (like bacteria and viruses) that cause infections or disease. The immune system consists of a network of cells (called leukocytes or white blood cells), tissues, and organs that work together to protect the body. The immune system can be broadly divided into two parts: innate immunity and adaptive immunity, each with distinct roles and cell types.
In this section we’ll go over how the immune system works in a general way while addressing key concepts that relate to infertility and IVF.
Innate immunity: The body’s first defense
Innate immunity is the first line of defense, responding quickly to any pathogen. This system is always on alert and responds in the same way to all threats.
- Physical Barriers: Skin and mucous membranes act as barriers to block pathogens from entering the body.
- Chemical Barriers: Substances like stomach acid and enzymes in saliva help destroy pathogens.
When a pathogen breaches these barriers, various immune cells take action:
- Neutrophils: These are the most common immune cells that rush to the infection site to engulf and destroy pathogens.
- Macrophages: Larger cells that also engulf and digest pathogens and dead cells. These cells also assist in activating the adaptive immune system.
- Natural Killer (NK) cells: These cells target and kill virus-infected cells and cancer cells.
- Dendritic Cells: These cells capture pathogens and present pieces of them to other immune cells, acting as a bridge to alert the adaptive immune system.
One of the key responses of innate immunity is inflammation, which is like setting off an alarm system. When tissues are injured or infected, they release chemical signals that increase blood flow and attract immune cells to the site. This results in redness, heat, swelling, and pain, which help isolate and eliminate the invaders and initiate tissue repair.
- Acute inflammation is a rapid and short-term response that resolves after the infection or injury is cleared.
- Chronic inflammation is a prolonged and persistent inflammatory response that can last for weeks, months, or even years, often leading to tissue destruction and disease. Chronic inflammation can be driven by persistent infections, autoimmune reactions where the immune system attacks the body’s own tissues, or prolonged exposure to harmful substances like tobacco smoke.
The innate immune system reacts immediately but in a non-specific way, meaning it doesn’t target specific invaders but attacks anything foreign. Now let’s look at the body’s more specific immune response.
Adaptive immunity: The body’s tailored defense
Adaptive immunity is like a specialized task force that comes into play if pathogens get past the initial defenses of the innate immune system. It takes a bit longer to respond but provides a very specific and effective defense to each pathogen.

This system remembers past infections and responds more effectively upon re-exposure to the same pathogen. It involves two main types of cells:
-
B Cells: These cells produce antibodies, which are like targeted missiles that lock onto specific invaders, neutralize them, or mark them for destruction.
- Plasma B cells: These cells produce large amounts of antibodies.
- Regulatory B cells: These cells control and suppress the immune response to prevent overreaction.
-
T Cells: These cells recognize and respond to infected cells.
- T helper cells (Th cells): These cells help activate other immune cells and direct the immune response.
- Cytotoxic T cells: These cells kill infected cells directly by making them self-destruct (apoptosis).
- T helper-17 (Th17) cells: These cells that play a crucial role in inflammation and autoimmune responses by producing the cytokine IL-17.
- Regulatory T (Treg) cells: These cells control and suppress the immune response to prevent overreaction. They can suppress Th17 cells, and the balance of Treg and Th17 cells is important for autoimmunity and inflammation.
T helper cells are particularly important in activating the adaptive immune response, and become activated by antigen-presenting cells like macrophages or dendritic cells. Antigen-presenting cells capture pathogens and present pieces of the pathogen (antigens) to T helper cells, which activates the T helper cell so it can alert other cells of the adaptive immune system, like B cells or cytotoxic T cells. Antigens don’t need to come from a pathogen — they can come from anything that triggers an immune response (usually foreign substances, but in the case of autoimmunity these antigens can be from the body itself).
Cytokines and Th1/Th2 cells
Depending on the way T helper cells are activated, they can become Th1 or Th2 cells. Th1 cells are a type of T helper cell that tend to activate cytotoxic T cells, and Th2 cells tend to activate B cells. Th1 and Th2 cells secrete chemical signals called cytokines to help activate these cells.
Th1 cytokines tend to be pro-inflammatory and Th2 cytokines tend to be anti-inflammatory and promote tissue repair. Other cells can also be polarized to be pro- or anti-inflammatory: M1 macrophages are pro-inflammatory and M2 macrophages are anti-inflammatory and promote tissue repair.
Here’s a list of some common pro- and anti-inflammatory cytokines:
- Interleukin-1 (IL-1) [Pro-inflammatory]
- Interleukin-6 (IL-6) [Pro-inflammatory]
- Interleukin-17 (IL-17) [Pro-inflammatory]
- Tumor Necrosis Factor-alpha (TNF-alpha) [Pro-inflammatory]
- Interferon-gamma (IFN-gamma) [Pro-inflammatory]
- Interleukin-10 (IL-10) [Anti-inflammatory]
- Transforming Growth Factor-beta (TGF-beta) [Anti-inflammatory]
- Interleukin-4 (IL-4) [Anti-inflammatory]
- Interleukin-13 (IL-13) [Anti-inflammatory]
The majority of immune cells secrete cytokines, and these chemical signals act as a form of communication that can change the behavior of cells. For example, macrophages can start secreting IL-1 to initiate and propagate inflammation. IL-1, together with other cytokines, can encourage T cells to become Th1 cells, which can then produce additional pro-inflammatory cytokines to amplify the inflammatory response.
The Th1/Th2 cytokine ratio can be measured as part of a patient’s reproductive immunology workup. This involve measuring Th1 cytokines like IL-1, IL-17, TNF-alpha and Th2 cytokines like IL-10 and IL-4 in the blood. A high Th1/Th2 ratio would indicate that there’s more Th1 cytokines, which is pro-inflammatory.
Wound healing: An example of the immune system in action
Now that we’ve discussed the basics of the immune system, let’s put it together with the example of wound healing. Here, a cut causes an injury, which introduces bacteria. The reason I’m using this example is because — believe it or not — there’s similarities between wound healing and embryo implantation.

When you get a cut or a scrape, the first thing your body does is try to stop the bleeding using platelets to form a clot. Along with platelets, mast cells also arrive in response to tissue damage and release histamine to make blood vessels more permeable, allowing other immune cells to enter the wound area.
After the injury, the body’s immune system jumps into action to protect against infection. Neutrophils are among the first to arrive at the scene. They attack and engulf bacteria or other foreign invaders and clear out dead cells. These cells create a very pro-inflammatory environment, which is crucial for this early phase of wound healing.
This pro-inflammatory environment attracts more immune cells to the site. Th1 cells are part of the adaptive immune system and help orchestrate this response along with M1 macrophages, which also clean up debris and fight infection. Th17 cells can also promote inflammation.
As the inflammation starts to resolve, thanks in part to regulatory T (Treg) cells, the body shifts to the next phase, known as the proliferative phase. This is where tissue repair starts. Anti-inflammatory M2 macrophages come into play and help to calm the inflammation and support tissue repair. Th2 cells also contribute by promoting healing processes and reducing inflammation.
During this repair phase, fibroblasts lay down collagen to begin to fill in the wound. Angiogenesis, the formation of new blood vessels, also occurs to ensure that the new tissue receives enough oxygen and nutrients.
Careful control of immune system is key to a successful pregnancy
When the embryo implants into the decidua (the thickened endometrium), it’s greeted by many different immune cells, including NK cells, macrophages and T cells.
These cells are crucial for pregnancy, and experiments that deplete these cells results in pregnancy loss in animal models (Mor et al. 2011). Liu et al. (2024) found that patients with low numbers of white blood cells before pregnancy had a higher chance of miscarriage (I review this study in my post Increases in immune cells associated with reduced risk of miscarriage).
So the role of immune cells in pregnancy is more about protecting the pregnancy rather than terminating it. The key is careful control of the immune system in maintaining a pregnancy! The first trimester is pro-inflammatory, the second is anti-inflammatory and the third is again pro-inflammatory.

The first trimester of pregnancy resembles an “open wound” that demands a strong pro-inflammatory response (Mor et al. 2011):
- The embryo breaks down the endometrial tissue to invade it, which is then encourages the development of a blood supply.
- This process recruits a large number of immune cells and requires substantial tissue reorganization and repair, much like what we saw earlier with the wound repair example. It’s possible that endometrial receptivity and the window of implantation is influenced by the specific immune cells present and their behavior.
- Inflammation that is too high during the first trimester may not be ideal, as shown by Li et al. (2023), where patients with the highest levels of inflammation around the time of egg retrieval had lower live birth rates and increased miscarriage risk. I reviewed this study in my post High systemic inflammation linked to worsened IVF pregnancy outcomes.
- Fun fact! Morning sickness is due in part to the large amount of inflammation during the first trimester.
The second trimester is anti-inflammatory (Bhagirath et al. 2021):
- During this time, the endometrium becomes enriched with macrophages and regulatory T cells (which ramp up during the first trimester, peak in the second, and then decrease in the third).
- Progesterone levels also increase, which leads to more Th2 cells and anti-inflammatory cytokines.
In the third trimester, delivery occurs, which again involves a pro-inflammatory state (Mor et al. 2011). This stage promotes contraction of the uterus and expulsion of the baby and placenta.
Careful control of the immune system is essential in embryo implantation and in maintaining a pregnancy. If the immune system is dysfunctional in anyway then this could lead to implantation failure or miscarriage.
Infertility diagnoses associated with the immune system
There are a number of infertility diagnoses that are associated with the immune system and unregulated inflammation. Let’s look at a few examples!
Uterine anomalies like endometrial polyps, hydrosalpinx, and uterine fibroids can disrupt the uterine environment. These conditions often involve local inflammation and immune dysregulation, making the uterus less receptive to embryo implantation and potentially contributing to RIF (Ebrahimi et al. 2024).
Endometriosis is characterized by the growth of endometrial tissue outside the uterus, leading to chronic inflammation and scarring in the pelvic area. The resulting pro-inflammatory state can interfere with multiple stages of the reproductive process, including embryo implantation (Ebrahimi et al. 2024). Macrophages have also been implicated in endometriosis, and have been associated with pain and the development of endometriosis (Zhang et al. 2022).
Chronic endometritis is a persistent bacterial infection in the endometrial lining that can cause chronic inflammation. This can lead to immune dysregulation and disrupt the balance of immune signals needed for embryo implantation (Ebrahimi et al. 2024).
Macrophages and the cytokines released by these cells have also been implicated in PCOS, mainly through inflammation (Zhang et al. 2022).
Immune cells involved in infertility and IVF
Natural killer (NK) cells
During early implantation, there are a large number of immune cells in the decidua — consisting of about 70% NK cells (Mor et al. 2017).
When it comes to NK cells in IVF, we usually are talking about two types:
- The peripheral blood NK cells (pbNK cells) – these are NK cells that are in the blood and are involved in killing virus infected cells.
- The uterine NK cells (uNK cells) – these are in the uterus and tend to promote implantation by creating a suitable environment.
- pbNK cells are generally not in the uterus, although it’s possible that pbNK cells can migrate into the uterus and turn into uNK cells (Carlino et al. 2008).
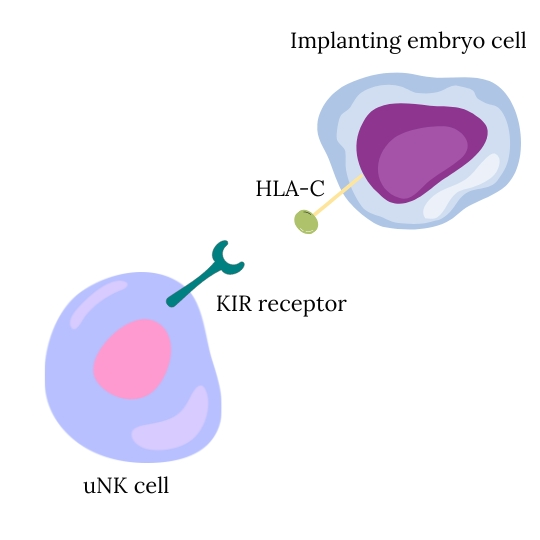
There are certain molecules on the surface of the uNK cell and the implanting embryo that can bind together to activate or inhibit uNK cells:
- On NK cells, these are called Killer cell immunoglobulin-like receptors, or KIR receptors.
- On the implanting embryos, these molecules are called human leukocyte antigen or HLA, with the major one being HLA-C.
Certain combinations seem to work better for implantation. As reviewed by Wasilewska et al. (2024), women with KIR AA whose embryo has HLA-C2 are at increased risk of RIF, but the opposite happens in women with KIR B receptors. There’s many types of KIR receptors on NK cells and many types of HLA molecules on implanting embryos, and the combination of all these signals is what dictates whether implantation will be supported or not. Because of all the variability, this leads to a highly individualized response to an implanting embryo.
A recent meta-analysis by Von Woon et al. (2022) combined 60 studies that looked at NK cells in women with RIF or RPL, and found:
- Higher levels of uNK cells in women with RIF.
- No difference in pregnancy outcomes in RIF/RPL women based on uNK cell levels.
- No association with pbNK and uNK cell levels in women with RIF/RPL.
- There was too much variability in the studies to draw conclusions on uNK cell activity.
For more information of NK cells, check my post NK cells in IVF.
Macrophages
Macrophages make up about 20% of the white blood cells in the endometrium (Mor et al. 2017), and there are two major types (based on the Th1/Th2 system described earlier):
- M1 macrophages: Pro-inflammatory macrophages that are dominant during the early stages of implantation.
- M2 macrophages: Anti-inflammatory and promotes tissue repair. They’re more common as pregnancy progresses, promoting a supportive environment for fetal development.
During early implantation, a mix of M1 and M2 macrophages are present, but as implantation and pregnancy continues, the environment shifts towards an M2-dominant state. An imbalance between M1 and M2 macrophages can disrupt the inflammatory environment needed for successful implantation.
Some studies (reviewed by Zhang et al. 2022) have shown an increase in CCL2 in RIF patients (CCL2 is a cytokine that can change macrophages to the M2 state). This might upset the balance of M1/M2 during early implantation that could lead to implantation failure.
Regulatory T cell (Treg) and Th17 cells
About 10-20% of immune cells in the decidua are T cells and 10-30% of these T cells are Treg cells (Robertson et al. 2018).
Treg cells are important for embryo and implantation for a number of reasons (Robertson et al. 2018):
- Tregs are crucial for establishing immune tolerance at the maternal-fetal interface, and allows the mother’s immune system to accept and support the genetically distinct embryo during implantation.
- While inflammation is crucial for the initial stages of implantation, this inflammation must be reduced and controlled for implantation to progress. Tregs seem to be important in this function, and is likely mediated through the generation of anti-inflammatory cytokines and M2 macrophages.
- Tregs facilitate the vascular changes needed to form the placenta and support implantation of the embryo into the uterine lining.
There is a balance between Th17 and Treg cells, with Th17 cells favoring inflammation and autoimmunity and Treg cells opposing this. Th17 cells can inhibit Treg cells, and vice-versa. An imbalance of Th17/Treg cells and of pro-/anti-inflammatory cytokines may be associated with implantation failure and miscarriage:
- Studies have shown that women with recurrent miscarriage show elevated inflammatory cytokines (IL-1B, TNF, IFN-γ) and decreased anti-inflammatory cytokines (IL-4, IL-6, IL-10, LIF, VEGF) in the endometrium (Robertson et al. 2018).
- Huang et al. (2021) found that the proportion of Treg cells and anti-inflammatory cytokines was lower in RIF patients, while Th17 cells and pro-inflammatory cytokines were elevated. This imbalance can lead to a more pro-inflammatory environment that may be prolonged and prevent implantation.
- A small study by Saifi et al. (2014) found that the ratio of Th17/Treg cells was tilted toward higher Th17 levels in patients with recurrent miscarriage.
- Pourmoghadam et al. (2020) found a low Th17/Treg ratio in women with RIF compared to patients without RIF. Patients who received PBMCs (to increase inflammation) and hCG had a higher live birth rate after embryo transfer, with lower miscarriage rates.
- Improper formation of the placenta can lead to miscarriage or adverse pregnancy outcomes like preeclampsia, which has been linked to low Treg numbers (Robertson et al. 2018).
Similar to Treg cells, regulatory B cells (Breg) also play a role in suppressing Th17 cells and modulating immune responses, with some links to RIF (reviewed by Ebrahimi et al. 2024).
Autoimmunity and autoantibodies
As mentioned earlier, antigens are substances that can trigger an immune response, such as from a pathogen or toxin. A specialized type of B cell, called a plasma cell, can produce antibodies that target the antigen to destroy it or block it in someway.
In some cases, people produce antibodies against their body’s own antigens. These are called autoantibodies and can lead to different autoimmune diseases like arthritis or lupus.
Having any kind of autoimmune disorder usually means there’s chronic inflammation in the body, and this might upset the balance needed for successful embryo implantation and pregnancy. It’s always important to discuss these things with your doctor and follow their recommendations.
Let’s look at a few examples of autoimmune disorders that are known to affect fertility.
Thyroid antibodies and thyroid autoimmunity
The thyroid gland regulates metabolism, growth, and development through the secretion of important hormones like thyroxine (T4) and triiodothyronine (T3). Thyroid hormones help to support normal ovarian function, follicle development, and the health of the endometrium, which is vital for embryo implantation and pregnancy maintenance (Vissenberg et al. 2015).
{kind=link}
{kind=link}
{kind=link}
Thyroid antibodies are autoantibodies that target thyroid proteins, like thyroid-peroxidase (anti-TPO) or thyroglobulin (anti-TG), that can potentially lead to damage of the thyroid and disrupt thyroid function. These antibodies are associated with adverse pregnancy outcomes such as preterm delivery and pregnancy loss, as well as infertility (Vomstein et al. 2021):
- Between 5-14% and 3-18% of pregnant women have either anti-TPO or anti-TG antibodies, respectively, and about 9.5% of women with a previous pregnancy loss have anti-TPO (Tanska et al. 2023).
- A 2019 meta-analysis found that patients with normal thyroid function and anti-TPO levels had a higher chance of preterm birth.
- A 2020 meta-analysis found that patients with thyroid autoimmunity and anti-TPO/anti-TG antibodies had an increased risk of pregnancy loss.
- While earlier studies linked thyroid autoimmunity to poorer embryo quality and lower success rates with IVF, recent research, reviews, and meta-analyses have not confirmed this (Tanska et al. 2023).
The negative effect of thyroid autoimmunity on fertility may be due to its co-occurrence with other autoimmune disorders (like antinuclear antibodies or antiphospholipid antibodies), its ability to lead to an imbalance in Th1/Th2/Th17/Treg activity, or thyroid hormone deficiency (Tanska et al. 2023).
Since patients with thyroid autoimmunity might not produce enough thyroid hormones, a common treatment is levothyroxine, which is a synthetic form of the thyroid hormone thyroxine. As stated by Tanska et al. 2023, four meta-analyses that only included RCTs didn’t find any evidence that levothyroxine improved pregnancy outcomes like miscarriage. “Although these observations require further analysis, the only beneficial effect of levothyroxine treatment in [thyroid autoimmune] women documented so far is prevention of hypothyroidism.”
Antiphospholipid antibodies
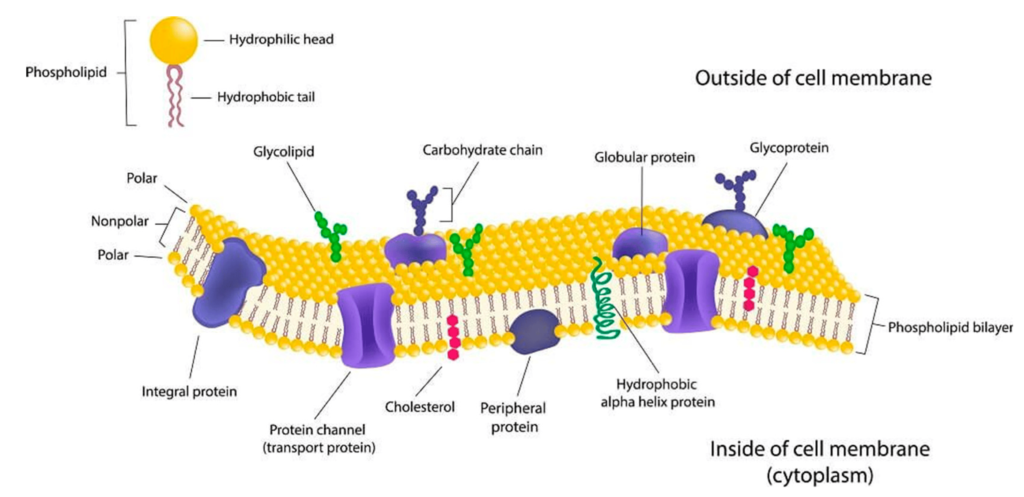
Antiphospholipid antibodies are autoantibodies that target phospholipids found in the cellular membrane of our cells, leading to blood clots and pregnancy complications.
People with antiphospholipid syndrome (APS) have a high amount of antiphospholipid antibodies. These antibodies and APS have been linked to infertility:
- APS is estimated to occur in 5-20% of RPL patients, although this may be overestimated (Vomstein et al. 2021).
- Studies have shown that people with APS might have trouble with embryo implantation, which may also occur even in patients without APS but who have antiphospholipid antibodies (Ebrahimi et al. 2024).
- A 2021 meta-analysis found that patients who had a failed IVF cycle had higher levels of antiphospholipid antibodies and higher miscarriage rates, with no change in clinical pregnancy or live birth rates.
Antinuclear antibodies
Antinuclear antibodies are autoantibodies produced against components of the nucleus that can be used to help diagnose certain autoimmune diseases. They also may be involved in infertility:
- A meta-analysis by Zeng et al. (2019) found that patients who had antinuclear antibodies were more likely to have reduced clinical pregnancy rates and implantation rates, and increased miscarriage rates (based on 11 studies).
Immunotherapy add-ons for IVF
Immunotherapies are treatments that suppress the immune system or specific aspects of the immune system like inflammation. NK cells are usually implicated in immune dysregulation and fertility problems, although immunotherapies don’t specifically target NK cells and are more broad in their effects.
Although patients with an autoimmune disorder may be receiving these treatments for their condition, in many cases immunotherapies are prescribed to patients without any indication of a pre-existing autoimmune disorder.
Generally, immunotherapies for routine use (ie. in patients without autoimmune disorders) don’t have strong supporting evidence backed by high quality RCTs. This has led to organizations like the the HFEA to not recommend their use, over concerns of safety and effectiveness. Likewise, ESHRE also doesn’t recommend their use along with the ASRM (based on their 2018 analysis). Common problems cited by these organizations include:
- RCTs don’t have a good sample size.
- Side effects aren’t addressed and some treatments may have potentially serious side effects.
- Multiple immunotherapies may be involved, making it hard to know which treatment is working or if it’s a combination effect.
- No universal standardization of testing (different tests can be used to establish a problem with the immune system) or treatment (different doses/timing of treatment).
- Patients included in studies may be defined too narrowly, making it hard to know if a treatment would work for the general public.
- The rationale for using some of these treatments is not grounded in what’s been established in biology (ie. uNK cells don’t attack and kill the fetus).
These treatments are often considered by patients with multiple failed cycles without any known immune disorders. Many of them report success with immunotherapies, and in some cases after many years of trying. It’s possible that these patients simply got lucky, or they have an underlying immune problem that hasn’t been diagnosed, or something else is going on! Maybe some patients just need these immunotherapies to “fine tune” their immune response to improve outcomes (for example, maybe there’s a bit too much inflammation that impairs implantation and an immunotherapy helps to bring it down to more ideal levels). Ultimately, better quality research is needed to see if these immunotherapies benefit the general public, or to find a specific group of patients that consistently benefit.
In terms of the overall effect of immunotherapies…A large retrospective study by Khairy et al. 2024 that combined different immunotherapies found a benefit in RIF with an underlying immunological issue. They used prednisolone, heparin, IVIG and intralipids, either alone or in combination. Multiple analyses in their study showed a benefit, but they didn’t have a group of patients with immunological problems that didn’t receive the treatment. There were other issues as well, and I’ve reviewed the study in my post RIF patients benefit from single or combination immunotherapy during IVF. I like this post also because it shares some details on the immune protocols used.
Now let’s look at some of the research on the effectiveness of single immunotherapies (not in combination with other immunotherapies). Research using a single immunotherapy is ideal because it tells us if that one particular treatment works (whereas it’s hard to say what’s working with multiple treatments).
One meta-analysis I’ll be referencing a bit is by Melo et al. (2022), which I review in my post Meta-analysis of commonly used IVF immunotherapies shows no benefit.
Aspirin
Low-dose aspirin is commonly used during IVF and may improve implantation by improving uterine blood flow and reducing inflammation.
- A 2022 meta-analysis found that aspirin didn’t improve live birth rates (6 RCTs).
- This meta-analysis reported no adverse effects, although aspirin is known to cause gastrointestinal disturbances and bleeding.
Heparin
Heparin, available as unfractionated and low-molecular-weight heparin (LMWH), may enhance IVF outcomes not only through its anticoagulant effects but also by influencing the implantation process.
- A 2022 meta-analysis found that heparin didn’t improve live birth rates (3 RCTs).
- This meta-analysis reports that the safety of heparin in pregnancy is well established.
Corticosteroids
Corticosteroids, like prednisone/prednisolone, are anti-inflammatory drugs that work by suppressing the immune system and reducing inflammation through inhibition of cytokine production and immune cell activity.
- A 2022 meta-analysis found that women who used corticosteroids didn’t show an improvement in live birth rate (5 RCTs).
- This meta-analysis reports that the use of corticosteroids can lead to insomnia and mild euphoria, and persistent use beyond the first trimester may lead to increased risk of infections or mental disorders in children.
- Sun et al. (2023) performed an RCT on RIF patients receiving 10 mg of prednisone and found no differences in clinical pregnancy, live birth or miscarriage rates. They found an increased risk of preterm deliveries with prednisone. I review this study in my post RCT finds no benefit for prednisone use among RIF patients.
Granulocyte colony-stimulating factor (G-CSF, Neupogen, Filgrastim)
G-CSF is a cytokine produced by different immune cells and tissues, and primarily functions in stimulating the proliferation of neutrophils. It might improve IVF outcomes by supporting embryo implantation and pregnancy.
- A 2022 meta-analysis found that intrauterine G-CSF improved live birth rates (5 RCTs), with women with a thin endometrium showing the most benefit.
- This meta-analysis reported fatigue, bone and muscle pain as adverse effects.
- Jinno et al. (2023) found that priming DOR patients with G-CSF before ovarian stimulation improved the cumulative live birth rate, with no adverse neonatal outcomes.
Intralipids
Intralipids are emulsified fat that is delivered intravenously. It’s believed to reduce the activity of NK cells and suppress inflammation.
- A 2022 meta-analysis found no improvement in live birth rate (2 RCTs).
- This same meta-analysis reported no adverse effects until higher doses were used, which led to increased infection risk, acute kidney injury, venous thromboembolism, allergic reactions, and fat embolism.
Intravenous immunoglobulin (IVIG)
IVIG is an intravenous infusion of human derived antibodies. It’s commonly used to treat autoimmune conditions and for chronic inflammatory conditions.
- A 2022 meta-analysis found no improvement in live birth rate (1 RCT), while several prospective studies found a benefit.
- Yamada et al. (2022) performed an RCT in women with RPL (no IVF was done) and found improved live birth rates with high dose IVIG.
Human Leukemia Inhibitory Factor (hLIF)
hLIF is a cytokine that may be involved in implantation.
- A 2022 meta-analysis found a decrease in live birth rate (1 RCT).
- The same meta-analysis found serious adverse effects (without being more specific).
Peripheral blood mononuclear cells (PBMCs)
PBMCs are collected from blood and include a variety of immune cells such as lymphocytes (T and B cells and NK cells), monocytes and macrophages. These cells are delivered to the uterus where they may improve implantation.
- A 2022 meta-analysis found an improvement in live birth rate (2 RCTs).
Conclusions
Successful embryo implantation and pregnancy rely on careful control of the immune system.
The immune system includes different cells, including macrophages, neutrophils, natural killer (NK) cells, B cells and T cells, which communicate through chemical signals to manage inflammation — a key response to infections or injuries.
Inflammation acts as the body’s alarm system, recruiting multiple immune cells to isolate and eliminate threats and begin tissue repair.
During embryo implantation, a controlled inflammatory response is needed. The first trimester is characterized by a pro-inflammatory environment, supported by T helper-1 (Th1) cells and M1 macrophages, with uterine NK cells creating a supportive environment for the embryo.
In the second trimester, this response shifts to an anti-inflammatory state, facilitated by Th2 cells and M2 macrophages, promoting tissue growth and fetal development. Regulatory T cells (Treg) play a crucial role in managing this shift and establishing immune tolerance of the embryo.
As the pregnancy progresses into the third trimester, the body returns to a pro-inflammatory state to prepare for delivery.
Imbalances in these immune responses are associated with recurrent implantation failure or recurrent pregnancy loss. Autoimmune conditions, where the immune system mistakenly attacks the body’s own cells, can also contribute to infertility.
Immunotherapies such as prednisone, intralipids and heparin aim to control immune responses to improve IVF outcomes. However, while these treatments show promise, better quality studies are needed to confirm their effectiveness for the general population.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Increases in immune cells associated with reduced risk of miscarriage
Increases in immune cells associated with reduced risk of miscarriage
 Study finds immune signature in endometrium of recurrent pregnancy loss patients
Study finds immune signature in endometrium of recurrent pregnancy loss patients
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 ASRI releases 2025 immune therapy guidelines for recurrent pregnancy loss
ASRI releases 2025 immune therapy guidelines for recurrent pregnancy loss
 NK cells in IVF
NK cells in IVF
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?