Aneuploid embryo success rates after transfer are very low, with about 1% leading to a live birth, likely due to undetected mosaicism after PGT-A rather than true whole chromosome aneuploidy.
Embryos labeled as aneuploid by PGT-A are usually not transferred, based on the assumption that they won’t lead to a successful pregnancy. Most clinics consider these embryos non-viable and usually discard them.
But what actually happens when these embryos are transferred? Can aneuploid embryos actually work?
This post focuses specifically on whole chromosome aneuploids, where an entire chromosome is missing or duplicated (for example, trisomy 21). These are different from segmental aneuploids, where only part of a chromosome is affected. Segmental aneuploids tend to behave differently and often have higher success rates, so they’re not included here. Check here to see posts about segmental aneuploids.
A small number of studies, along with rare case reports, have looked at outcomes after transferring embryos labeled as fully whole chromosome aneuploid. In this post, I’ve pulled together the available data to better understand how often these embryos lead to a live birth and what those rare cases might mean.
This post reflects the current evidence as of mid-2026 and will be updated as new data becomes available.
For more background reading, check my Complete guide to PGT-A.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Studies examining the transfer of aneuploid embryos
All of the studies included here used next-generation sequencing (NGS), which has been the dominant method for PGT-A since around 2013. Earlier methods like microarray have lower resolution and different classification thresholds, so results from those are harder to compare and are not included in the main analysis. Read more in my post: How PGT-A testing has evolved (1990’s to today).
1) Wang et al. (2021) performed a prospective, nonselection study where embryos were chosen by morphology and PGT-A results were revealed after transfer.
- Number of aneuploids transferred: 44
- Number of live births: 2 (monosomy 16; monosomy 22)
- Live birth rate: 4.5% (2/44)
- Miscarriage rate: 75% (6/8 pregnancies ended in loss)
2) Tiegs et al. (2021) performed a prospective, blinded nonselection study where embryos were transferred before PGT-A results were known.
- Number of aneuploids transferred: 102
- Number of live births: 0
- Live birth rate: 0% (0/102)
- Miscarriage rate: 100% (24/24 pregnancies ended in loss)
- Read more in my post: IVF outcomes following aneuploid embryo transfer
3) Barad et al. (2022) transferred mosaic and aneuploid embryos prospectively. The embryos had already been labeled as abnormal (aneuploid or mosaic) by PGT-A at other clinics, and were transferred knowing this.
- Number of aneuploids transferred: 76 (original report); 84 in a later reanalysis
- Number of live births: 0 (NGS-only analysis); 1 in the original dataset (later found to be from microarray)
- Live birth rate: 0% (NGS-only)
- Miscarriage rate: unclear
-
Other notes:
- An earlier version of this study was published under Yang et al. (2021)
- Later analysis (Gleicher et al. 2023) clarified that the one live birth came from an embryo tested with microarray, not NGS.
- Madjunkov et al. (2026) reanalyzed the data as NGS-only and reported ~84 embryos with 0 live births. The increase from the original 76 is not clearly explained, but may be due to pooling with earlier data (from Yang et al. 2021).
- The dataset mixes different testing methods, and it’s not always clear which embryos used which
- Read more in my post: 144 “abnormal” (aneuploid/mosaic) embryos and their outcomes
4) Madjunkov et al. (2026) examined outcomes after transferring embryos labeled as aneuploid using NGS-based PGT-A in a nonselection design (embryos transferred without knowledge of PGT-A results).
- Number of aneuploids transferred: 70
- Number of live births: 0
- Live birth rate: 0% (0/70)
- Miscarriage rate: 100% (9/9 pregnancies ended in loss)
Overall success rates after transferring aneuploid embryos
Combining all the studies from above:
- Transfers: 300 (44 + 102 + 84 + 70)
- Live births: 2
- Live birth rate: 0.7% (2/300)
Most individual studies reported no live births from whole chromosome aneuploid embryos.
Overall, aneuploid embryo success rates after transfer are very low, with a live birth rate about 1% based on current data.
There are other studies that report on live births from whole chromosome aneuploids, but weren’t included in the overall success rate calculation:
- Tise et al. (2025) reported a case of healthy euploid twin girls born after transfer of aneuploid embryos. However, this was a case report, not a study that transferred many aneuploid embryos and tracked all outcomes. It was published because the outcome was successful and unusual, so including it in the overall success rate could overestimate how often these transfers actually lead to live birth.
- Shen et al. (2022) also reported a live birth from an embryo later classified as aneuploid, but only one whole chromosome aneuploid was identified, and the embryo was tested years after transfer using stored DNA samples, making it harder to compare directly with the studies above.
Why do aneuploid embryos work?
Before we look at why aneuploid embryos might work, it’s important to address why they shouldn’t work.
Why aneuploid embryos shouldn’t work
If an embryo is truly uniformly aneuploid (meaning all cells carry the same chromosomal error), it shouldn’t implant and lead to a healthy pregnancy without those errors.
This is because every cell would have the same problem, so the baby would be expected to have those chromosomal abnormalities too. When a healthy baby is born without them, it suggests the embryo may not have been fully aneuploid.
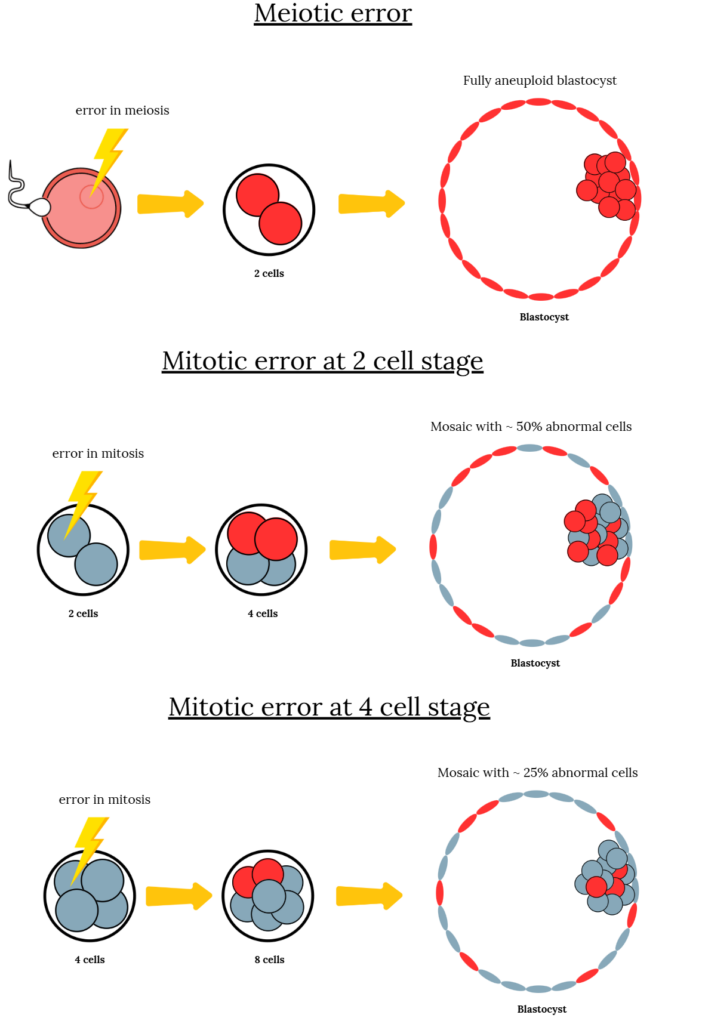
In fully aneuploid embryos, the error usually comes from the egg or sperm and affects every cell. This is known as a meiotic error, because it occurs during the formation of the egg or sperm. In contrast, a mitotic error happens after fertilization and affects only some cells, resulting in a mosaic embryo that has a mix of normal and abnormal cells.
Why aneuploid embryos sometimes appear to work
There are a few possible explanations:
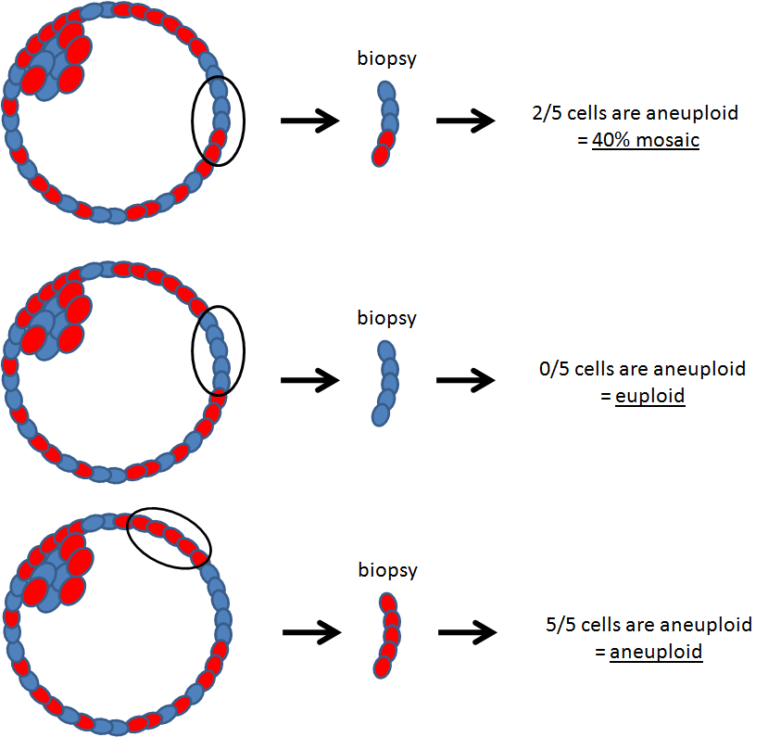
The aneuploid embryo is actually mosaic. PGT-A tests only a small number of cells, which might not be fully representative of the embryo in some cases. It’s possible that, by chance, a biopsy of a mosaic embryo only samples abnormal cells and misses some of the normal cells, giving the appearance that the embryo is fully aneuploid.
Mosaic embryos can self-correct, where the mosaic corrects itself of the abnormal cells it carries. This may be due to the normal cells outgrowing the aneuploid cells, or the aneuploid cells may be partitioned to the trophectoderm (leaving the ICM normal).
Supporting this, a systematic review by Marin et al. (2021) found that when embryos initially labeled as aneuploid were retested, about 18.6% were no longer classified as aneuploid. However, other studies have found higher concordance rates (around 97–98%), suggesting that while most aneuploid results are consistent, some may not be fully aneuploid. This could help explain rare successful outcomes. Read more in my post: Does a PGT-A biopsy match the rest of the embryo?
Technical limitations. PGT-A involves DNA amplification and sequencing from a very small sample. Thresholds are used to classify embryos as aneuploid or euploid, which may not always reflect an embryo that is truly 100% aneuploid. There can also be noise in the data, for example from lower-quality biopsy samples, making accurate classification more difficult.
Rare technical issues like DNA contamination can also distort PGT-A results, sometimes making normal embryos appear abnormal. Read more in my post: DNA contamination is rare but can affect PGT-A results.
Rare or external explanations. In a small number of cases, sample mix-ups or embryo mislabeling could occur, leading to the transfer of an embryo that isn’t actually aneuploid. It’s also possible, though uncommon, that an unassisted conception occurs if intercourse happens around the time of transfer.
Conclusion
Across multiple studies, embryos labeled as whole chromosome aneuploid have a very high chance of failing to implant or miscarrying. Live births are rare, but not impossible, with a rate of about 1%.
It’s not always obvious why an aneuploid embryo can lead to a successful pregnancy, but many likely reflect the limitations of PGT testing.
More data is needed to better understand these cases. One example is the ongoing Stanford-led study following transfers of embryos labeled as aneuploid or mosaic, which aims to track outcomes over time. You can learn more at clinicaltrials.gov/study/NCT04109846.
Want to read more about aneuploid embryo success rates?
A new case report describes the healthy birth of dizygotic twin girls from embryos labeled as aneuploid by PGT-A, highlighting the limitations of embryo testing and the need to reconsider strict discard protocols. Read more.
Researchers in a 2022 study reported on the outcomes of 144 "abnormal" embryos, consisting of aneuploids and mosaics, finding a single live birth with an aneuploid and more favorable results with mosaics. Read more.
Researchers in a 2020 study performed a clinical trial and transferred aneuploid embryos, finding that no whole chromosome aneuploids led to a live birth, while segmental aneuploids did. Read more.
Aneuploid embryos, with an abnormal number of chromosomes, are a major cause of miscarriages, often linked to maternal age and errors in meiosis. In this post, we'll explore what chromosomes and aneuploidy are, how meiosis errors cause aneuploidy, and the factors contributing to these errors, including age, genetics and mitochondrial dysfunction. Read more.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.