This post traces the evolution of PGT-A testing in IVF, from early FISH and microarray methods to modern NGS and emerging technologies like nanopore sequencing, highlighting how each advancement improved accuracy, speed, and embryo assessment.
PGT-A is used in IVF to identify embryos with the wrong number of chromosomes, an issue that becomes more common with age and is a major cause of miscarriage. The goal is to reduce miscarriage risk and improve live birth outcomes, especially in patients with advanced maternal age, recurrent pregnancy loss, or repeated implantation failure.
This post walks through the evolution of PGT-A, using a review by Oltramare et al. (2025) and de la Paz et al. (2024) as a guide.
For more background on PGT-A, check my complete guide to PGT-A.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
The earliest version of PGT-A tested embryos on day 3, during the cleavage stage. A single cell (blastomere) was removed for analysis, but this approach often failed to reflect the genetic status of the entire embryo. Many day 3 embryos show mosaicism (Sciorio et al. 2020), where some cells are normal (euploid) and others are abnormal (aneuploid). Testing just one cell increases the risk of a false result.
Eventually, testing shifted to day 5 blastocysts. By sampling several cells from the trophectoderm, the results became more reliable and better reflected the overall chromosomal status of the embryo.
Alongside changes in biopsy timing, the testing platforms themselves have gone through several phases:
- 1990s–2008: Fluorescence in situ hybridization (FISH)
- 2008–2013: Microarrays (aCGH and SNP arrays)
- 2013–present: Next-generation sequencing (NGS)
- 2016–present: Early clinical research into third-generation platforms like nanopore sequencing
Each leap forward brought improvements in speed, resolution, and the ability to detect things like mosaicism and segmental abnormalities.
Now let’s walk through each era of PGT-A, summarizing how the field has changed, what each method could and couldn’t do, and what it all means for IVF patients today!
Table of Contents
PGT-A’s evolution: The FISH era (1990s-2008)
FISH was the first method used for PGT-A in the 1990s. It involves tagging chromosomes with fluorescent dyes and looking at them under a microscope. The problem was that early FISH could only check a handful of chromosomes at once, often 5 to 7 and usually including 13, 15, 16, 18, 21, 22, X, and Y (Macville et al. 1997).
That left a lot of room for missed abnormalities!
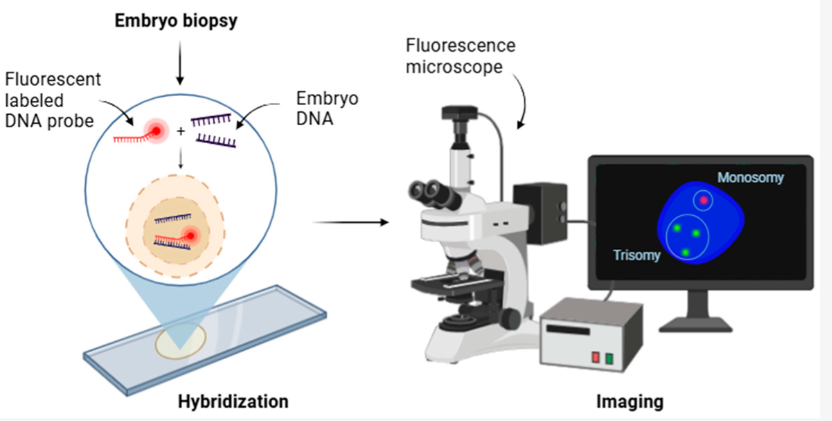
To test more chromosomes, some labs did two rounds of FISH, but this was labor-intensive and still limited in scope. FISH also couldn’t reliably detect mosaicism unless it affected the specific chromosomes being tested, and even then the accuracy was questionable.
Studies on women with advanced maternal age or recurrent implantation failure didn’t find clear benefits, with one trial showing that FISH-based PGT-A actually reduced live birth rates (Mastenbroek et al. 2007), while another showed no benefit (Blockeel et al. 2008).
FISH gave us our first glimpse into embryo chromosomal status, but its inability to test all chromosomes or detect mosaicism accurately meant it wasn’t suitable for clinical PGT-A.
PGT-A’s evolution: The microarray era (2008-2013)
Since embryo biopsies yield only a tiny amount of DNA, a key advancement in PGT-A was the use of whole genome amplification (WGA). WGA is a technique that takes the limited genetic material from just one or a few cells and creates millions of copies, essentially photocopying the entire genome so it can be studied in detail. Without this step, there wouldn’t be enough DNA to run tests on all 24 chromosomes.
Once amplified, the DNA can be analyzed using different platforms, including aCGH, SNP arrays, qPCR or NGS. Each method has its own strengths, but all rely on WGA to generate the amount of material needed for reliable analysis.

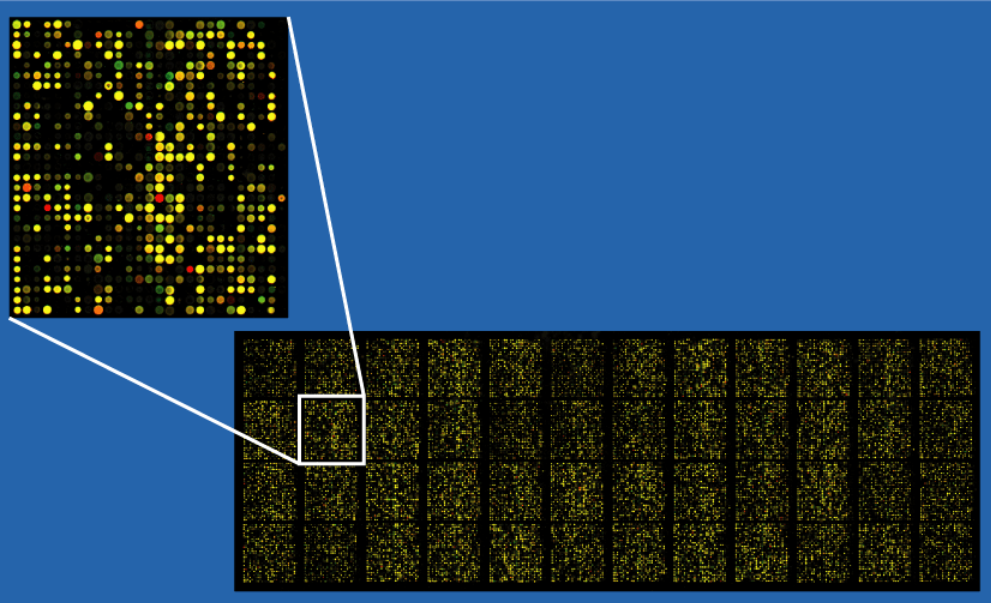
This era introduced microarrays, a technology that uses a small chip covered in thousands of short DNA fragments, like a grid of molecular Velcro. When the embryo’s amplified DNA is applied, it binds to matching spots on the grid, generating signals that help detect missing or extra chromosome material.
{kind=link}
Microarrays were the first technologies that enabled full chromosome screening in embryos. One early method was aCGH (array comparative genomic hybridization), which compares embryo DNA to a normal reference sample. Each is labeled with a different fluorescent dye, and any imbalance in signal suggests a gain or loss of DNA in a chromosomal region.
- Detects: Aneuploidy (missing or extra chromosomes) and mosaicism (only if 40–60% of cells are abnormal)
- Resolution: 6–10 Mb (megabases) — meaning it can detect gains or losses larger than 6 to 10 million base pairs
- Time required: 9 to 30 hours
- Cost: Around $5000 USD
- Common embryo stage tested: Cleavage stage (day 3, inner cell mass) and blastocyst stage (day 5, trophectoderm biopsy)
SNP arrays, another type of microarray, analyze hundreds of thousands of single nucleotide polymorphisms (tiny sequence variations scattered throughout the genome). Instead of comparing to a reference sample, SNP arrays often use parental DNA to interpret the embryo’s genetic profile.
- Detects: Aneuploidy, mosaicism (down to 50%), and polyploidy.
- Resolution: About 6 Mb — can detect slightly smaller chromosomal abnormalities than aCGH, but still limited to larger-scale events
- Time required: About 24 hours
- Common embryo stage tested: Cleavage stage (day 3) and blastocyst stage (day 5)
During this same period, some clinics adopted qPCR (quantitative polymerase chain reaction) as a faster and more affordable alternative to microarray-based PGT-A. Instead of scanning the entire genome using a microarray chip, qPCR focused on amplifying and measuring specific DNA regions per chromosome. This limited approach made the process fast (often quick enough for a fresh transfer) and relatively inexpensive, but could miss segmental changes or unbalanced translocations.
Together, these methods helped shift embryo testing from day 3 to day 5, when more cells could be biopsied and results were more accurate.
Some studies showed promising outcomes. One found that using aCGH increased live birth rates from 32.8% to 54.1% in women with advanced maternal age (Lee et al. 2019). But others showed more modest improvements or no significant difference (Harton et al. 2013).
Microarrays and qPCR were a major step forward in speed, accuracy, and scope of PGT-A. But they still had key limitations, including difficulty in detecting low-level mosaicism or segmental abnormalities, and high cost. These gaps eventually led to the adoption of next-generation sequencing (NGS), which was more sensitive and cost-effective per sample.
PGT-A’s evolution: The next-generation sequencing (NGS) era (2013-present)
Currently (2025), next-generation sequencing (NGS) is the dominant method for PGT-A because it offers higher resolution, faster turnaround, and lower costs per embryo than older techniques. NGS can detect aneuploidy, polyploidy, mosaicism (even when present in just 20% of sampled cells) and segmental aneuploidy (large deletions or duplications).
- Detects: Aneuploidy, mosaicism (as low as 20%), and polyploidy
- Resolution: 1–3 Mb — can detect smaller chromosomal changes than aCGH or SNP arrays, down to 1 million base pairs
- Time required: 15 to 24 hours
- Cost: Much lower, typically $41 to $502 USD
- Common embryo stage tested: Blastocyst stage (day 5, trophectoderm biopsy only — not used for day 3)
Importantly, NGS allowed a better understanding of mosaicism, where embryos have a mix of normal and abnormal cells (read more about mosaics in my post on mosaic embryos).
NGS-based PGT-A works by sequencing short fragments of DNA from the embryo biopsy and comparing them to a reference genome. Too many reads suggest extra DNA (like a trisomy), too few suggest missing DNA (like a monosomy), and intermediate values may suggest mosaicism. You can see an example of NGS-based PGT-A data below. If you want to learn more about how NGS works and how to interpret raw PGT-A data, check here.

Not all NGS platforms work the same. In PGT-A, a platform refers to the specific combination of sequencing technology, reagents, software, and algorithms used to perform PGT-A and interpret the results. Illumina’s MiSeq (VeriSeq) and Thermo Fisher’s Ion ReproSeq are two of the most widely used in PGT-A, each with its own proprietary chemistry, read size, amplification method, and algorithm for calling results. Some are faster, more automated, or better at detecting mosaicism at certain levels.
PGT-A using NGS has been associated with lower miscarriage rates and higher live birth rates in some RCTs, especially among women with advanced maternal age:
- Munne et al. (2019) found no overall difference in pregnancy or miscarriage rates between transferring a euploid embryo or the best-looking one. However, in women aged 35–40, euploid transfer led to higher ongoing pregnancy rates (51% vs 37%). I reviewed this study in my post PGT-A doesn’t improve success rates in good prognosis patients.
- Yan et al. (2021) found no difference in cumulative live birth after up to three transfers with or without PGT-A, but miscarriage rates were lower with PGT-A (8.7% vs 12.6%). I reviewed this study in my post PGT-A vs embryo grading: results of a 2021 clinical trial.
But there are still limitations of NGS:
- Mosaicism detection isn’t perfect and can vary between platforms. An embryo labeled aneuploid on one platform might be classified as mosaic on another, depending on the platform’s algorithm, cutoff for mosaicism, and resolution.
- During DNA preparation, some parts of the genome may get copied more than others (called amplification bias), or fail to copy at all (called dropout). This can make it seem like there’s too much or too little DNA in certain areas, which may lead to incorrect results.
- Some embryos fail to yield usable results (2–3%).
- The platforms themselves are expensive (up to $650,000 USD for the equipment) (Quail et al. 2012). Because of this, most IVF clinics don’t perform the NGS testing in-house. Instead, embryo biopsies are usually sent to external PGT labs equipped with these machines and the bioinformatics expertise needed to analyze the large sequencing datasets.
PGT-A’s evolution: Third generation sequencing and nanopore sequencing (2016-present)
A variety of new sequencing technologies are now emerging that may reshape how PGT is done, dubbed “third generation sequencing.”
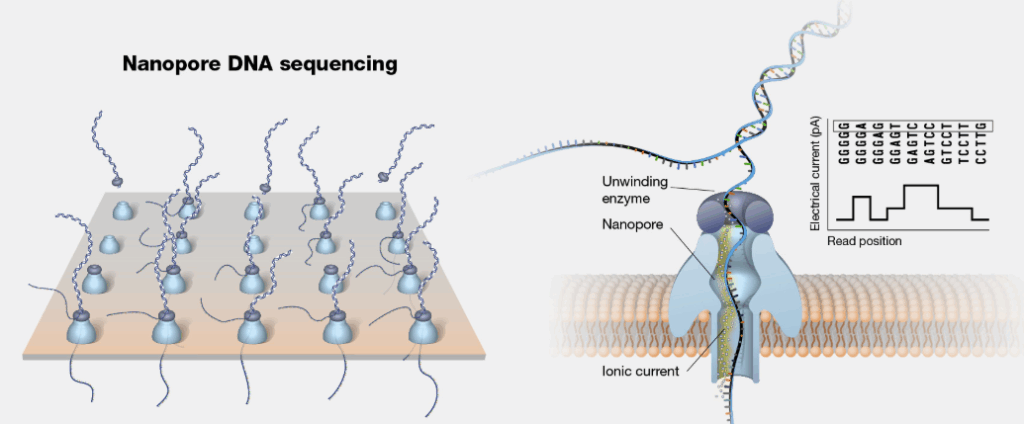
One example is nanopore sequencing, which offers faster results, real-time data, and dramatically lower equipment costs (about $3000 USD).

Instead of cutting DNA into tiny fragments like NGS, nanopore methods thread whole strands through a microscopic pore and read the sequence in real time. This allows faster processing, possibly within the same day of embryo biopsy, and might eliminate the need to freeze embryos while waiting for results.
Early studies suggest nanopore sequencing is 98–99% concordant with NGS for aneuploidy and mosaicism detection, cheaper per sample (as low as $50–$200), and feasible for in-house use by IVF clinics. Read more in my post New “STORK” method makes PGT-A faster and cheaper.
Still, most work is early and implementation will require validation, staff training, and reliable workflows. But it’s a promising direction, especially for reducing turnaround times and allowing clinics to perform PGT-A in-house.
Non-invasive PGT-A methods under development
Non-invasive PGT-A methods aim to reduce the risks and limitations of traditional embryo biopsy by analyzing DNA or embryo development without removing cells for a biopsy (de la Paz et al. 2024):
- Cell-free DNA (cfDNA) in blastocoel fluid (BF) can be aspirated with minimal disruption, but DNA quantities are low and amplification success is inconsistent. Some studies show moderate concordance with trophectoderm biopsy, but results vary widely.
- cfDNA in spent culture medium (SCM) offers a fully non-invasive approach, with greater DNA yield than BF. However, results are often affected by contamination from maternal cells or lab reagents. Concordance with invasive PGT-A ranges from 15% to 100% across studies.
- Artificial intelligence (AI) tools analyze embryo development using time-lapse imaging. Systems like KIDScore, iDAScore, Life Whisperer, and newer models like ERICA and STORK-A aim to predict ploidy and implantation potential by analyzing morphokinetics, embryo morphology, and clinical data.
While still under development, these non-invasive PGT-A methods offer the potential for safer, faster, and less technically demanding ways to assess embryo quality.

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to PGT-A (PGS testing)
Complete guide to PGT-A (PGS testing)
 Complete guide to mosaic embryos
Complete guide to mosaic embryos
 Study finds differences in euploid, live birth rates among PGT-A testing labs
Study finds differences in euploid, live birth rates among PGT-A testing labs
 Does a PGT-A biopsy match the rest of the embryo?
Does a PGT-A biopsy match the rest of the embryo?
 Can a mosaic embryo result in a normal baby?
Can a mosaic embryo result in a normal baby?
 A look at how PGT-A results change with age, using data from over 86,000 biopsies
A look at how PGT-A results change with age, using data from over 86,000 biopsies
 ASRM’s 2024 committee opinion on the use of PGT-A
ASRM’s 2024 committee opinion on the use of PGT-A
 Chromosomal errors in IVF: What is aneuploidy and what causes it?
Chromosomal errors in IVF: What is aneuploidy and what causes it?