
After a failed first IVF cycle, researchers found that switching ovarian stimulation protocols was linked to a reduced chance of another cancellation, with factors like age, diagnosis and smoking status also contributing to success.
About 10% of first IVF cycles are cancelled, mainly due to low ovarian response (not enough follicles).
The study reviewed here wanted to see if there were any factors that contribute to success or another cancellation in a second IVF cycle after the first cycle was canceled.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This study uses 2014-2017 data from the SART CORS database, which is based on ~90% of US fertility clinics.
- Patients were included if they had a first IVF cycle that was canceled (no egg retrieval), followed by a second cycle. The second cycle was either canceled or resulted in an egg retrieval/transfer.
- More than 80% of the second cycles were done within a year of the first.
- The cancellation reason for the first and second cycle was often due to “low response.” A low response means the patients didn’t respond well to ovarian stimulation and didn’t have many follicles. There are more strict definitions (ie. Bologna criteria, POSEIDON criteria), but this study didn’t use those definitions and relied on what the doctor listed as the reason for cancellation in SART CORS. So there’s likely variability in how different doctors defined “low response,” and this is a limitation of the study.
- All the live births reported in this study were from the second cycle, and were from the first transfer (either fresh or frozen).
What were the reasons for cycle cancellation?
In this study, there were 13,340 patients who had a canceled first IVF cycle and then went on to have a second IVF cycle, with 3112 who had another canceled cycle and 10,228 who didn’t. About half of the patients had DOR, with about 20% over the age of 40.
On the SART CORS database (where this data comes from), the doctors indicated a number of possible reasons for cancellation, which you can see below:
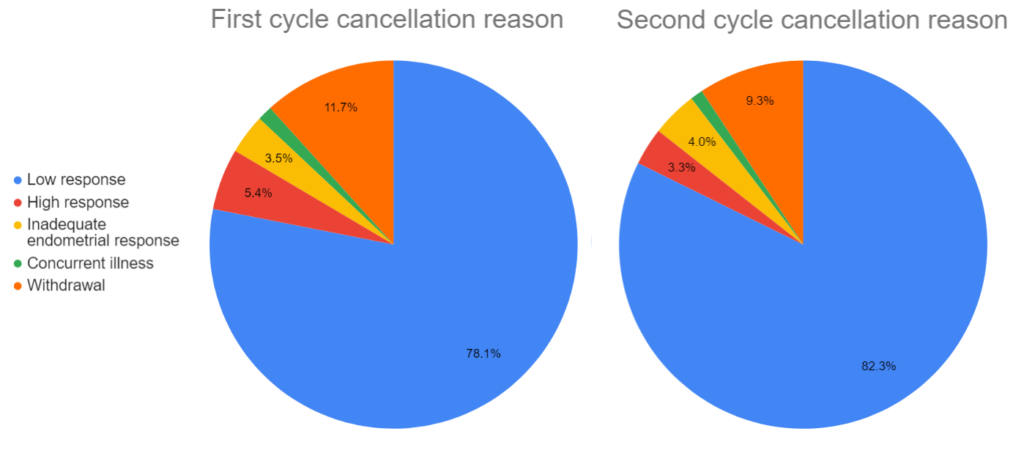
Most patients canceled due to a “low response,” meaning they didn’t respond well enough to the ovarian stimulation to have a retrieval (not enough follicles). Patients with a high response likely had too many follicles and OHSS was a concern, so the cycle was canceled. Although it wasn’t explained, I’m assuming cancellations due to inadequate endometrial response is for patients who were planning on a fresh transfer but their endometrium wasn’t looking ideal. Patients who withdrew from treatment either had psychological or financial concerns, a family emergency or other reasons.
A look at patients who had a canceled first IVF cycle, live birth in second cycle
In this study, there were 13,340 patients who had a canceled first IVF cycle and then went on to have a second IVF cycle, with 3112 who had another canceled cycle and 10,228 who didn’t. Of these 10,228 patients, 5646 had an embryo transfer, with 1860 live births (32.9% live birth rate).
The researchers compared the characteristics of the 1860 patients that had a live birth, to see who was more likely to have a live birth:
- Younger patients were more likely to have a live birth (compared to patients aged <35: patients aged 35-37 had a 45% lower odds of live birth; 38-40 had a 68% lower odds; 41-42 had a 89% lower odds; 43+ had a 91% lower odds).
- BMI made no difference.
- Patients who were ever smokers had a 24% lower odds of live birth.
- Certain races had a lower odds of live birth (compared to white patients: Asian patients had a 42% lower odds of live birth; Black 46% lower odds; no difference with Latino or mixed race). The authors note that the race data is limited, due to missing data.
- Certain diagnoses were associated with live birth (patients with male infertility had a 26% increased odds; diminished ovarian reserve had a 44% decreased odds; no change for endometriosis, PCOS, tubal factor, uterine, recurrent pregnancy loss or unexplained). This was statistically adjusted for age, BMI, smoking status and race.
- Patients with a max historical FSH >10 mIU/ml had a 41% reduced odds of live birth (vs those with 10 mIU/ml or less).
- Patients with a last known AMH 1.0 ng/ml or less had a 16% reduced odds of live birth.
- Patients who cancelled their first cycle because of low response had a 28% reduced odds of live birth. This was statistically adjusted for age, BMI, smoking status, race and AMH.
A look at patients who had a canceled first IVF cycle, canceled second cycle
In this study, there were 13,340 patients who had a canceled first IVF cycle and then went on to have a second IVF cycle, with 3112 who had another canceled cycle and 10,228 who didn’t.
The researchers compared the characteristics of the 3112 patients that had a second canceled cycle, to see who was more likely to have a second canceled cycle:
- Older patients were more likely to have a second canceled cycle (compared to patients aged <35: patients aged 35-37 had a 68% increased odds of a second canceled cycle; 38-40 had a 131% increased odds; 41-42 had a 161% increased odds; 43+ had a 219% increased odds).
- Certain diagnoses were associated with having a second canceled cycle (patients with PCOS had a 27% reduced odds of a second canceled cycle; DOR had a 89% increased odds; no change for male infertility, endometriosis, tubal factor, uterine, recurrent pregnancy loss and unexplained). This was statistically adjusted for age, BMI, smoking status and race.
- Patients with a max historical FSH >10 mIU/ml had a 90% increased odds of a second canceled cycle (vs those with 10 mIU/ml or less).
- Patients with a last known AMH 1.0 ng/ml or less had a 183% increased odds of a second canceled cycle.
- Patients with a change in their stimulation protocol had a 12% reduced odds of a second canceled cycle.
- Patients who cancelled their first cycle because of low response had a 36% increased odds of another canceled cycle. This was statistically adjusted for age, BMI, smoking status, race and AMH.
Outcomes when patients changed ovarian stimulation protocols
Since these patients had a canceled first IVF cycle, many of them had a second cycle using a different ovarian stimulation protocol in the hope that changing the protocol would improve outcomes. The researchers note that this is the largest study comparing protocol changes, so how did they do?
- There were less 0.36 less eggs retrieved, and 0.29 less fertilized eggs.
- There was a 14% lower odds of having a cancellation.
- There was a 17% increase in the odds of a live birth.
- This data was statistically adjusted for age, BMI, smoking status, race, AMH and infertility diagnosis.
There were three types of ovarian stimulation protocols used in these patients: agonist flare, agonist suppression and antagonist. They compared outcomes for patients that switched or didn’t switch protocols between the first and second cycle, with the results below. Note that these are relative to the group that didn’t switch (ie. there were 3.25 more eggs retrieved when patients switched from agonist flare to agonist suppression, compared to patients that didn’t switch from agonist flare and used it a second time). This data was statistically adjusted for age, BMI, smoking status, race, AMH and infertility diagnosis.

The data above was for all the patients, but they also looked at patients who had their first cycle cancelled due to poor response. The result were essentially the same, except patients who switched from agonist suppression to antagonist saw a 41% decrease in the odds of cancellation.
More details: There were 6434 patients that changed their protocols and 6701 patients who didn’t. There were mostly no differences in their patient characteristics, but there were differences in the amount of gonadotropins used (4105 IU of FSH vs 3695 IU, for the changed vs same protocol groups). They adjusted for gonadotropin dosing in a statistical model and found this didn’t change their results, but they note that about 20% of cycles didn’t report gonadotropin dosing — this is a limitation of the study.
Conclusion
Younger patients, non-smokers, and those with male infertility were more likely to have a live birth, while older age, higher FSH levels, low AMH, certain racial backgrounds (Asian and Black), and having a cycle previously canceled due to low response were associated with lower odds of live birth. The authors note that the race data is limited, due to missing data.
Patients who were older, had diminished ovarian reserve, higher FSH levels, or low AMH were more likely to have a second canceled IVF cycle, while those with PCOS were less likely to experience a second cancellation.
Patients who switched ovarian stimulation protocols were less likely to have a cancellation (agonist flare to agonist suppression), and more likely to have a live birth (between agonist suppression and antagonist protocols). Certain switches were also associated with a increases/decreases in the number of retrieved eggs. This was true even after controlling for gonadotropin dosing.
ESHRE guidelines recommend patients start with an agonist suppression or antagonist protocol, instead of an agonist flare, for both normal and poor responders. This agrees somewhat with the data in this study. Recent studies have shown a benefit with agonist suppression and antagonist cycles over agonist flare in poor responders (links below).
A number of limitations were mentioned for this study:
- Non-specific definition of poor responder.
- Unclear if benefits from switching protocols are from the switch, or from the doctor proceeding with the cycle anyway (to avoid another canceled cycle).
- They were unable to directly compare the two cycles in the same patient (limitation of SART CORS database).
- SART CORS doesn’t include more modern ovarian stimulation protocols (estrogen priming, duostim, etc).
- Limited data on gonadotropin dosing.
For a related post, check out my post Study examines impact of changing ovarian stimulation protocol. They found some differences in IVF outcomes, but these patients didn’t experience a canceled cycle like here.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (3 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Study finds poor ovarian responders have no further live births after 4 cycles
Study finds poor ovarian responders have no further live births after 4 cycles
 IVF and pregnancy outcomes in women with low AMH (≤0.3 ng/ml), by age
IVF and pregnancy outcomes in women with low AMH (≤0.3 ng/ml), by age
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles
 Impact of delayed treatment on IVF outcomes
Impact of delayed treatment on IVF outcomes
 Study examines impact of ovarian stimulation on egg quality
Study examines impact of ovarian stimulation on egg quality
 Comparing IVF outcomes from cycles with low AMH
Comparing IVF outcomes from cycles with low AMH
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 Examining live birth rates in IVF cycles with 5 or less follicles
Examining live birth rates in IVF cycles with 5 or less follicles