Researchers in a 2022 meta-analysis published in Human Reproduction Update, found that growth hormone (omnitrope) showed improved endometrial function and reproductive outcomes in poor responders and women with a thin endometrium, but not in normal responders.
Growth hormone (GH) is secreted by the pituitary gland and leads to synthesis of insulin-like growth factor 1 (IGF-1) in the liver. IGF-1 receptors are present on egg cells and the surrounding granulosa and theca cells in the follicle, and can assist in the process of egg maturation. For this reason, GH is often used during ovarian stimulation for poor responders (as Omnitrope) and may improve the quantity and quality of eggs retrieved (Hart 2019).
It also has a possible benefit on the endometrium, such as increasing endometrial thickness in poor responders or in those with recurrent implantation failure, as well as improving pregnancy outcomes (Shang et al. 2022). However a consensus on dosage, the route and timing of administration, and who really benefits from its use isn’t clear.
In this summary, Shang et al. (2022) performed a meta-analysis using 25 RCTs and 2424 women who used GH. The majority of studies were done in women with poor ovarian response (POR), however they also performed an analysis on studies with normal responders, as well as those with a thin endometrium.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Live birth rates
Women who used GH were more likely to have a live birth compared to those who didn’t (16.5% vs 10.4%, 9 studies, 945 participants, odds ratio [95% CI]: 1.67 [1.13-2.49]). The quality of evidence was reported as very low.
Clinical pregnancy rates
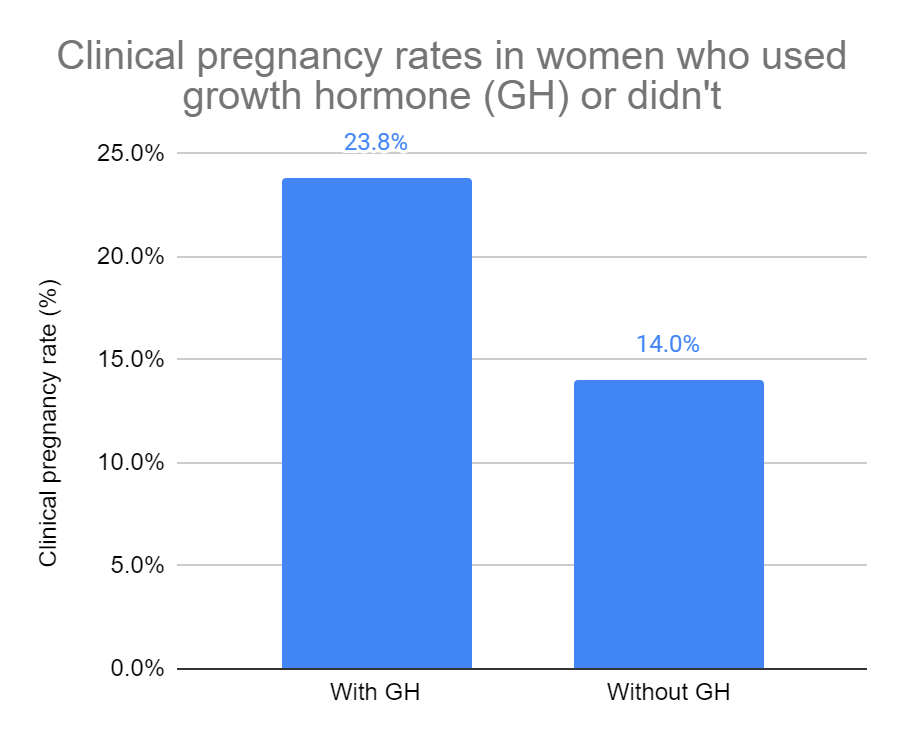
Women who used GH were more likely to have a clinical pregnancy compared to those who didn’t (23.8% vs 14.0%, 16 studies, 1593 participants, odds ratio [95% CI]: 1.97 [1.43-2.72]). Remember these are mostly poor responders, so the rates are a bit lower. The quality of evidence was reported as low.
They also did a subgroup analysis and found that the best results came when patients used <5 IU/day of GH, during the follicular phase of the previous cycle (until trigger) and used a GnRH agonist short protocol.
Miscarriage rates
They found no statistically significant differences in terms of miscarriage and GH based on 8 studies. The quality of evidence was reported as low.
Endometrial thickness
Women who used GH had on average a 0.38 mm thicker endometrium compared to those who didn’t use GH (10.52 mm vs 10.16 mm, 9 studies, 1121 participants, mean difference [95% CI]: 0.38 [0.18-0.59]). The quality of evidence was reported as moderate.
They also did a subgroup analysis and found that the best results came when patients used <5 IU/day of GH, during the follicular phase of the previous cycle (until trigger) and used a GnRH agonist long protocol.
Number of mature eggs retrieved
Women who used GH had on average 1.62 more mature eggs retrieved compared to those who didn’t (10 studies, 1262 participants, mean difference [95% CI]: 1.62 [1.05-2.19]). The quality of evidence was reported as very low. The best results were seen when women used 5-10 IU/day, during the luteal phase of the previous cycle (until trigger).
Adverse effects
Nine studies looked at adverse effects of GH. Two studies found slight edema and infant health issues in both GH and control groups, with no other reported events in the remaining studies.
Impact of GH on women with a thin endometrium
They evaluated 4 studies that included 354 patients with a thin endometrium that used GH and found:
- The odds of clinical pregnancy increased 2.71 times with GH
- Miscarriage rates didn’t change
- Endometrial thickness increased by 1.48 mm in women who used GH
- No difference in rate of high quality embryos
Based on 3 studies (261 participants) women who used GH had increased odds of having a multilayered endometrium (2.67 times higher) and visible blood flow (5.84). The quality of evidence was reported as moderate.
Impact of GH on normal responders
The majority of participants in these studies were poor ovarian responders. They identified two studies that included normal responders and found no differences in live birth rate or the number of eggs retrieved. The quality of evidence was reported as very low.
Overall, this meta-analysis found that in poor responders, GH improved live birth rates, clinical pregnancy rates and endometrial thickness, with best responses using dosages <5 IU/day, beginning in the follicular phase of the previous cycle and using a GnRH agonist long protocol. In women with a thin endometrium, GH improved endometrial thickness, pattern and blood flow as well as clinical pregnancy rates. In normal responders, there weren’t enough studies to draw a conclusion.
The authors point out that the overall quality of evidence presented was moderate to very low, and caution should be taken when considering these results, particularly live birth rates. Safety data was inadequate also, and more studies are needed to address this.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Growth hormone (omnitrope) increases number of eggs retrieved in updated meta-analysis
Growth hormone (omnitrope) increases number of eggs retrieved in updated meta-analysis
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Improving egg quality with supplements
Improving egg quality with supplements
 Evidence-based recommendations from ESHRE for 27 IVF add-ons
Evidence-based recommendations from ESHRE for 27 IVF add-ons
 Intraovarian PRP results in more eggs retrieved, but no improvement in egg quality
Intraovarian PRP results in more eggs retrieved, but no improvement in egg quality
 Meta-analysis of commonly used IVF immunotherapies shows no benefit
Meta-analysis of commonly used IVF immunotherapies shows no benefit
 Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
 RCT finds no change in birth rates for standard or ERA-timed euploid transfer
RCT finds no change in birth rates for standard or ERA-timed euploid transfer