
Researchers in a 2024 study performed an RCT and found that intraovarian PRP resulted in an increased number of eggs retrieved in patients with poor ovarian response, although these eggs weren’t more likely to become blastocysts or be euploid after PGT-A and resulted in fewer pregnancies.
Platelet rich plasma (PRP) is rich in growth factors and platelets that may have regenerative properties and has been used for different applications in IVF. One way is for it to be injected directly into the ovaries, which is thought to improve egg numbers and quality. This study compared patients who had intraovarian PRP injections vs those who had a saline (placebo) injection. They compared the number of eggs collected, and the quality of these eggs (by seeing if they were more likely to form blastocysts or euploids).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a double-blind, randomized controlled trial that took place in 2021 at a single IVF center in Spain.
- Patients were predicted poor ovarian responses (POR) and had diminished ovarian reserve, including patients classified as group 3 or group 4 by the POSEIDON criteria (AMH <1.2 ng/ml; check glossary for more info).
- Patients were all having their first cycle.
- Patients had 3 consecutive egg retrievals, then ICSI was performed and embryos were tested by PGT-A, with only a single euploid being transferred.
- PRP was prepared during the follicular phase of the first ovarian stimulation by collecting 15 ml of blood and centrifuging it to isolate the plasma layer. This layer was processed and injected into both ovaries after the first egg retrieval. A placebo PRP injection was also performed, which involved a saline injection into both ovaries. Patients and doctors were blinded as to who received PRP vs the placebo.
- The primary outcome was the total number of mature eggs retrieved after the 3 egg retrievals.
In terms of sample size, they performed a power analysis and determined that they needed 29 patients to detect an increase of 2 mature eggs. They recruited 60 patients, with 30 to receive PRP and 30 to receive the placebo. One of them dropped out, so there were 29 patients in the placebo group. Yes, there weren’t many patients, but there were enough to see if there was a difference in at least 2 eggs retrieved!
In terms of baseline characteristics, there were no differences between the PRP and placebo group in terms of: age (average was 37.59), AMH levels (0.70 ng/ml), AFC (3.90), BMI and group 3 (28%) or group 4 (72%) POSEIDON criteria patients.
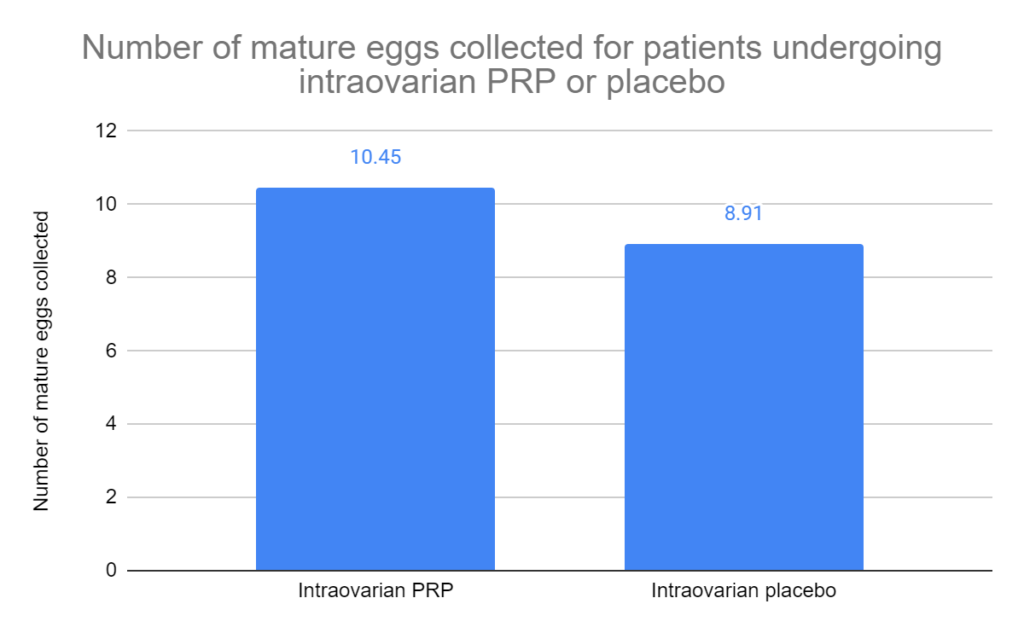
Intraovarian PRP increases number of eggs retrieved
In this study, patients had 3 consecutive egg retrievals with either an intraovarian PRP injection or a saline injection (placebo) after the first egg retrieval, and counted the total number of mature eggs collected.
The intraovarian PRP group collected a total average of 10.45 mature eggs, while the placebo group collected 8.91 mature eggs (average difference [95% CI]: 1.54 [0.42-2.66]; p= 0.008).
They reported the number of mature eggs collected for each of the 3 egg retrievals (PRP vs placebo):
- First retrieval: 2.55 vs 2.69 (no difference).
- Second retrieval: 4.18 vs 3.27 (no difference).
- Third retrieval: 5.27 vs 4.15 (p= 0.029).
When they looked at differences between the first and second (or third) cycle, they also found differences:
- For PRP, there was an increase in eggs from the first vs the second cycle (2.55 vs 4.18, p= 0.005) and for the first vs the third cycle (2.55 vs 5.27, p< 0.001).
- For the placebo, there was an increase for only the first vs the third cycle (2.69 vs 4.15, p= 0.001).
This is interesting because it shows that both PRP and the placebo resulted in more eggs in consecutive cycles. This suggests that the mechanical effect of the intraovarian injection itself is capable of leading to an increase in eggs, although slightly more with PRP. In case you’re wondering, the average time between retrieval 1 and 2 was 24.32 days and between 2 and 3 was 25.92 days.
No increase in number of blastocysts or euploids after intraovarian PRP
After the 3 consecutive egg retrievals, the eggs from the first two retrievals were thawed (average survival 85%) and combined with the 3rd retrieval, then ICSI and PGT-A were performed. Here’s a breakdown of the IVF outcomes (PRP vs placebo):
- Similar number of blastocysts (1.90 vs 2.43, p= 0.449).
- Similar blastocyst conversion from eggs (~44%).
- Same number of euploids (0.81). The % of patients with euploids was also similar (43% vs 53%, p= 0.606).
A single euploid was transferred, and here are the pregnancy outcomes (PRP vs placebo):
- Lower clinical pregnancy rates for the PRP group (27% vs 60%, p= 0.018).
- No difference in miscarriages (12% vs 28%, p= 0.628).
- No difference in full term pregnancies (aka live births) (23% vs 43%, p= 0.170).
So there doesn’t appear to be any improvements in egg quality, at least as far as the ability of the fertilized egg to turn into a blastocyst/euploid. It’s also strange that there was a lower pregnancy rate (half!), but this is a secondary outcome and the study wasn’t powered to detect differences in pregnancy outcomes, so this result is less reliable.
Conclusions
This study found a slightly higher number of mature eggs after 3 consecutive egg retrievals with PRP vs placebo in patients with POR. It’s not clear if this increase is clinically significant.
A higher number of eggs were collected after cycle 3 vs cycle 1 for both the PRP group and the placebo group, suggesting that the mechanical effect of injecting the ovary itself (ovary damage) led to an increase in mature eggs collected.
Besides ovarian damage, it’s possible that some other aspect is at play here, for example gonadotropins exposure from previous cycles that might have an impact on subsequent cycles. They probably didn’t consider it at the time, but it would have been a good idea to have another control that didn’t have any ovarian injections to evaluate this!
Besides the number of eggs collected, there didn’t seem to be any improvements in the quality of the eggs: the eggs weren’t more likely to convert to blastocysts, and the blastocysts weren’t more likely to be euploid.
There was also a lower pregnancy rate from the euploids transferred in the PRP group.
Despite some studies showing a benefit for PRP (referenced below), there doesn’t seem to be any effect of “ovarian rejuvenation” here, which is sometimes used to describe PRP. Instead, the authors believe that PRP, and mechanical damage of the ovary itself, might lead to follicle activation that resulted in more eggs retrieved.
Overall, there doesn’t seem to be much benefit for PRP based on this study, as the slight increase in numbers may not be worth it. However, it’s hard to know if there’s a benefit unless we can see outcomes in patients without any kind of ovarian injection. But even then, this improvement may be due to the mechanical effect of damaging the ovary by injection, and not the PRP itself.
The authors point out issues with intraovarian PRP, particularly the lack of standardization in dosing and preparation, and describing its mechanism of action. Without standardization, this makes it difficult to draw conclusions between studies.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (5 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
Meta-analysis combines results of 12 intrauterine, intraovarian PRP studies
 Meta-analysis combines 38 studies on treatments for diminished ovarian reserve
Meta-analysis combines 38 studies on treatments for diminished ovarian reserve
 Meta-analysis shows growth hormone improves endometrial function
Meta-analysis shows growth hormone improves endometrial function
 Growth hormone (omnitrope) increases number of eggs retrieved in updated meta-analysis
Growth hormone (omnitrope) increases number of eggs retrieved in updated meta-analysis
 CoQ10 and other supplements improve IVF outcomes in women with ovarian aging
CoQ10 and other supplements improve IVF outcomes in women with ovarian aging
 Large trial examines impact of growth hormone on IVF success
Large trial examines impact of growth hormone on IVF success
 AMH levels by age and how it relates to diminished ovarian reserve (DOR)
AMH levels by age and how it relates to diminished ovarian reserve (DOR)
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles