A 2025 study shows that segmental abnormalities detected by PGT-A in the trophectoderm don’t always match the ICM, suggesting that these embryos may still be viable for transfer.
PGT-A is used to prioritize embryos with a normal number of chromosomes (euploid) for transfer. But sometimes, results show a segmental abnormality, meaning only a small part of a chromosome is gained or lost.
Unlike embryos with whole-chromosome aneuploidy, which are typically deprioritized due to higher risk of pregnancy loss, there is little guidance on whether to transfer embryos with segmental aneuploidy.
Most PGT-A labs classify them as abnormal and won’t transfer them, but studies have shown that these embryos can result in healthy live births.
One of the challenges with PGT-A is that it typically samples the trophectoderm (TE), not the inner cell mass (ICM), which forms the fetus. A new study by Cheng et al. (2025) analyzed donated blastocysts, including some with segmental aneuploid results, to see if the results from the TE matched the ICM. The goal was to understand whether these embryos should always be ruled out for transfer.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
The researchers analyzed 175 blastocysts donated by 89 patients, which originally tested as follows:
- Segmental aneuploid: 36
- Segmental mosaic: 60
- Whole chromosome aneuploid: 52
- Whole chromosome mosaic: 14
- Euploid: 13
These donated embryos were thawed and biopsied a second time—this time from the inner cell mass (ICM), which forms the fetus.

The table below shows how often the inner cell mass results matched the original trophectoderm results.
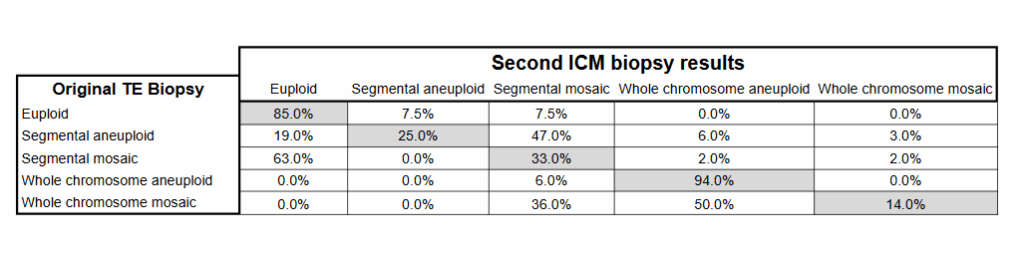
For embryos that originally tested as euploid or whole chromosome aneuploid in the TE, the ICM result usually matched:
- 85.0% of embryos that were euploid in the TE were also euploid in the ICM
- 94.0% of embryos with a whole chromosome aneuploidy in the TE also had a whole chromosome aneuploidy in the ICM
This means PGT-A results for euploid and whole chromosome aneuploid embryos are usually consistent with the ICM.
But the results were less consistent when the original biopsy was a segmental aneuploidy, a segmental mosaic, or a whole chromosome mosaic.
- Only 25.0% of embryos with segmental aneuploidy in the TE also had segmental aneuploidy in the ICM
- 33.0% of embryos with segmental mosaicism in the TE also had segmental mosaicism in the ICM
- 14.0% of embryos with whole chromosome mosaicism in the TE also had whole chromosome mosaicism in the ICM
These low match rates suggest that many embryos diagnosed as segmental or mosaic in the TE may actually have different results in the ICM. About two-thirds (63.0%) of segmental mosaics had a euploid ICM! And 19.0% of segmental aneuploids were euploid. These results raise questions about whether these embryos should be automatically excluded from transfer.
Conclusions
This study shows that when an embryo is labeled as having a segmental abnormality, the result may not reflect what’s happening in the ICM. About 1 in 5 embryos diagnosed with segmental aneuploidy and around 2 in 3 with segmental mosaicism had a normal ICM and could be viable. In contrast, euploids or whole chromosome aneuploids were highly likely to have the same result in the ICM.
The authors write that these mismatched results for segmental abnormalities may be due to natural mosaicism, technical testing issues, or the embryo correcting itself over time. Because of this, some embryos with segmental abnormalities could be considered for transfer, especially if there are no euploids available and ideally after genetic counseling.
The authors suggest a second biopsy might help in some cases, especially when a key region is affected, but caution that can risk harming the embryo.
Here’s some additional posts you might want to check out on Remembryo:
- Segmental aneuploid embryos after PGT-A lead to healthy live births — Researchers in 2024 report on live births after segmental aneuploid transfers, finding that they have similar rates as high level mosaic segmental aneuploids.
- Segmental aneuploids: the main source for PGT-A false positives? — Researchers in a 2022 study found that some segmental aneuploids, that only have a partial chromosomal abnormality, might not be aneuploid after all.
- IVF outcomes following aneuploid embryo transfer — Researchers in a 2020 study performed a clinical trial and transferred aneuploid embryos, finding that no whole chromosome aneuploids led to a live birth, while segmental aneuploids did.
- Ranking 1,000 mosaic embryo transfers — Researchers in a 2021 study compared outcomes from 1,000 mosaic embryo transfers, consisting of high and low level, as well as whole chromosome or segmental mosaics.
-
Does a PGT-A biopsy match the rest of the embryo? — Evidence up to 2022 shows that a single PGT-A biopsy is highly concordant (similar) with the rest of the embryo when the embryo is aneuploid or euploid, but not when it’s mosaic or segmental.
Related studies
These additional studies were referenced by the authors of the paper and haven’t been covered on Remembryo. They may be helpful if you’re exploring this topic further. This section is available for paid subscribers.

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Segmental aneuploids: the main source for PGT-A false positives?
Segmental aneuploids: the main source for PGT-A false positives?
 Segmental aneuploid embryos after PGT-A lead to healthy live births
Segmental aneuploid embryos after PGT-A lead to healthy live births
 IVF outcomes following aneuploid embryo transfer
IVF outcomes following aneuploid embryo transfer
 Trophectoderm and ICM biopsies match depending on the abnormality
Trophectoderm and ICM biopsies match depending on the abnormality
 Does a PGT-A biopsy match the rest of the embryo?
Does a PGT-A biopsy match the rest of the embryo?
 Mosaicism much more common than previously thought, using more sensitive PGT-A technique
Mosaicism much more common than previously thought, using more sensitive PGT-A technique
 More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic
More sensitive PGT-A test shows that nearly all blastocysts, fetal tissues are mosaic
 Embryos labeled aneuploid by PGT-A lead to healthy euploid twins
Embryos labeled aneuploid by PGT-A lead to healthy euploid twins