
Researchers in a 2023 study compared PGT-A outcomes for patients with different diagnoses, including advanced maternal age (AMA), recurrent implantation failure (RIF), recurrent pregnancy loss (RPL) and severe male factor (SMF).
I recommend you check out the glossary term for per retrieval vs per transfer to understand the difference, because that will be discussed here.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including the number of patients and their characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This is a retrospective cohort study that took place between 2019 and 2022 at a single IVF center in South Korea.
- Patients with AMA were 38 or older.
- Patients with RIF had no confirmed clinical pregnancies after at least 3 transfers.
- Patients with RPL had 2 or more miscarriages before 20 weeks.
- Patients with SML had azoospermia (obstructive/nonobstructive) and sperm concentration less than 5 million/ml, 40% motility, 4% morphologically normal sperm.
- One or two euploid or untested embryos were transferred.
In terms of the sample size, there were:
- AMA (233 patients; 289 as control).
- RIF (130 patients; 266 as control)
- RPL (80 patients; 132 as control)
- SML (77 patients; 161 as control)
In terms of baseline characteristics, for each group the control group was younger and had more embryos transferred. Unfortunately, they made no effort to control for this (by statistical adjustment, for example). This is a limitation of the study. The upside here is that we expect the control group to have a higher success rate (because they’re younger and transferred more embryos) — so if the PGT-A group is still higher, and this is statistically significant, we can be extra confident that PGT-A is better than no PGT-A.
Here are the average ages/number of embryos transferred for each group (PGT-A vs non-PGT-A):
- AMA (41.2 vs 40.5; 1.2 vs 1.6)
- RIF (37.9 vs 35.1; 1.2 vs 1.4)
- RPL (37.1 vs 34.7; 1.2 vs 1.3)
- SMF (38.2 vs 34.2; 1.2 vs 1.4)
Instead of live births, this study uses ongoing pregnancy/live births (OP/LB). Researchers use this occasionally because they want to publish a study quickly and don’t want to wait for all the pregnant patients to have a live birth. They combine the number of live births with those still pregnant past 20 weeks. You can think of it as live birth, to keep it simple.
Outcomes in patients with advanced maternal age (AMA), with or without PGT-A
For PGT-a vs non-PGT-A patients with AMA (average age 41.2 vs 40.5), there was an increase in per transfer clinical pregnancy and OP/LB rates and a decrease in miscarriage rates (54.0% vs 37.4%, p= 0.004; 42.0% vs 21.8%, p< 0.001; 16.7% vs 34.3%, p= 0.001). For per retrieval OP/LB there was no difference (p= 0.286).

For reference (PGT-A vs non-PGT-A):
- Number of egg retrieval cycles (233 vs 289).
- Number of transfer cycles per number of egg retrievals (100/233 vs 289/289).
- Number of miscarriages per clinical pregnancy (9/54 vs 37/108)
Outcomes in patients with recurrent implantation failure (RIF), with or without PGT-A
For PGT-a vs non-PGT-A patients with RIF, there was an increase in per transfer clinical pregnancy and OP/LB rates (61.0% vs 44.4%, p= 0.004; 47.0% vs 28.6%, p< 0.001). There no differences in miscarriage rates (p= 0.073) or for per retrieval OP/LB (p= 0.126).

For reference (PGT-A vs non-PGT-A):
- Number of egg retrieval cycles (130 vs 266).
- Number of transfer cycles per number of egg retrievals (100/130 vs 266/266).
- Number of miscarriages per clinical pregnancy (8/61 vs 29/118)
Outcomes in patients with recurrent pregnancy loss (RPL), with or without PGT-A
For PGT-a vs non-PGT-A patients with RPL, there was an increase in per transfer OP/LB rates and a decrease in miscarriages (49.1% vs 24.2%, p< 0.001; 16.7% vs 50.0%, p< 0.001). There no differences in per transfer pregnancy rates (p= 0.200) or for per retrieval OP/LB (p= 0.093).

For reference (PGT-A vs non-PGT-A):
- Number of egg retrieval cycles (80 vs 132).
- Number of transfer cycles per number of egg retrievals (57/80 vs 132/132).
- Number of miscarriages per clinical pregnancy (6/36 vs 35/70)
Outcomes in patients with severe male factor (SVM), with or without PGT-A
For PGT-a vs non-PGT-A patients with SVM, there were no differences in per transfer pregnancy and OP/LB rates, miscarriage rates, or per retrieval OP/LB rates (p= 0.121; p= 0.072; p= 0.074; p= 0.897).
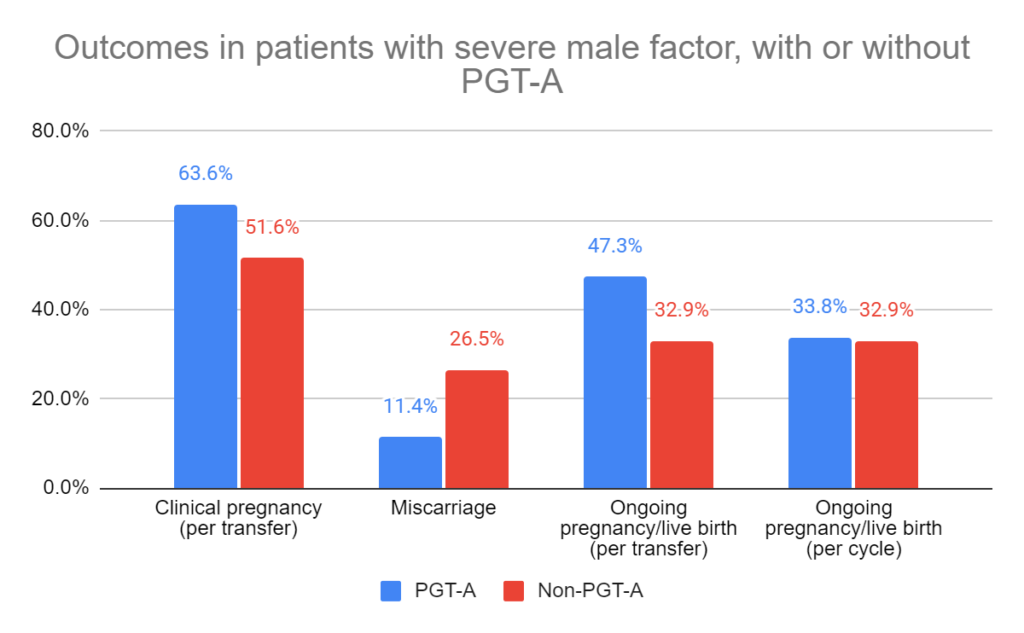
For reference (PGT-A vs non-PGT-A):
- Number of egg retrieval cycles (77 vs 161).
- Number of transfer cycles per number of egg retrievals (55/77 vs 161/161).
- Number of miscarriages per clinical pregnancy (4/35 vs 22/83)
Conclusions
For AMA:
Increase in pregnancies
Increase in OP/LBs
Decrease in miscarriage
For RIF:
Increase in pregnancies
Increase in OP/LBs
No change in miscarriage
For RPL:
No change in pregnancies
Increase in OP/LBs
Decrease in miscarriage
For SMF:
No change in pregnancies
No change in OP/LBs
No change in miscarriages
There were also no changes for any of the “per retrieval” OP/LBs. This tells us that patients who started an egg retrieval had the same chance of a live birth, whether they had PGT-A or not. What changes is potentially avoiding the transfer of non-euploids that may fail to implant or miscarry.
It’s unfortunate this study didn’t better control for age and the number of embryos transferred. For the SMF group in particular, there was the largest gap in age between PGT-A and non-PGT-A groups (about a 4 year difference). The non-PGT-A group also transferred more embryos (1.4 vs 1.2). Younger patients who transfer more embryos will have a higher chance of success, and if this was better controlled we may have seen a difference with PGT-A.
This study notes that their results align with other studies examining outcomes in PGT-A vs non-PGT-A patients, although it’s hard to know how thorough they were in their search for related references. They may have decided to just reference similar studies. Feel free to check out them out below.
Related studies
There were a number of studies referenced that you might want to check out, as shown below (8 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
Meta-analysis combines 74 studies to examine factors linked to euploid transfer success
 ASRM’s 2024 committee opinion on the use of PGT-A
ASRM’s 2024 committee opinion on the use of PGT-A
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Pilot study shows improved IVF outcomes after spindle transfer in women with poor egg quality
Pilot study shows improved IVF outcomes after spindle transfer in women with poor egg quality
 Euploid embryos show reduced implantation potential with advancing maternal age
Euploid embryos show reduced implantation potential with advancing maternal age
 Study performs genetic analysis on over 3,200 miscarriages
Study performs genetic analysis on over 3,200 miscarriages
 Study evaluates PGT-A outcomes for good prognosis patients, based on age
Study evaluates PGT-A outcomes for good prognosis patients, based on age