
A 2025 study found that transferring two good quality day 5 blastocysts increased the risk of miscarriage in singleton pregnancies compared to single embryo transfer, suggesting that transferring two good quality embryos may raise the risk of losing both, even if only one implants.
In double embryo transfer (DET), transferring two embryos can lead to either a multiple pregnancy if both implant or a singleton if only one implants or the other fails early. In singleton pregnancies after DET, a failed embryo may trigger inflammation that harms the surviving embryo, possibly increasing the risk of miscarriage or later complications.
This post is a summary of a study by Wang et al. (2025), who looked at whether DET increases the risk of pregnancy loss in singleton pregnancies compared to single embryo transfer (SET). In other words — In a DET, if only one embryo implants and grows, could the other embryo somehow interfere with the healthy one and cause the pregnancy to fail?
I’m going to simplify it even more because this is super important to understand for this study!
The study compared two groups:
- People who had a SET with a singleton pregnancy (only one gestational sac)
- People who had a DET, but ended up with a singleton pregnancy (only one gestational sac).
In the DET group, one of the two embryos either didn’t implant at all or implanted briefly but didn’t continue, because only a single gestational sac was seen.
The researchers wanted to know:
- Is miscarriage more likely in singleton pregnancies that started with two embryos compared to those that started with one?
- If so, does the quality of the embryos transferred make a difference?
The results of this study can help us better understand if transferring a second embryo can influence the development of the first (implanted) embryo.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This is a retrospective cohort study that took place between 2017 and 2022 in a hospital in China.
- Inclusions: Singleton pregnancies (detected by a single fetal heartbeat), FET cycles.
- Exclusions: Vanishing twin cases, history of spontaneous abortion or uterine malformation, chromosomal abnormalities, etc. Vanishing twins were excluded because previous data suggests an increased miscarriage risk, and the researchers wanted to focus on true singletons (with only gestational one sac ever seen) to test if transferring two embryos still raises risk through early, undetected embryo loss.
- Good quality blastocysts were defined as being day 5 and having expansion 4 or greater with quality AA, AB, BA or BB. A non-good blastocyst was day 5 or 6, with expansion 4 or greater, with quality AC, CA, BC or CB.
- Primary outcome was clinical pregnancy loss.
In terms of sample size, there were 2448 singleton pregnancies split up into three groups based on what was transferred during the FET:
- Day 3 embryo transfer (SET n= 153, DET n= 591).
- Double blastocyst transfer (mixed good and non-good quality) (SET n= 279, DET n= 281)
- Double blastocyst transfer (good quality) (SET n= 962, DET n= 182)
In terms of baseline characteristics, there were some differences but they were statistically adjusted in their analysis (variables adjusted include the number of oocytes retrieved, female age at oocyte retrieval, infertility duration, infertility cause, type of infertility, female BMI, semen DFI, previous transfer cycle, protocols of endometrial preparation, and embryo quality). About 85% of FET cycles in this study were from women <35 years old.
Double embryo transfer increases risk of pregnancy loss in singleton pregnancies
Alright! There isn’t much data in this study, but what they’re showing is pretty interesting.
In this study, the researchers compared pregnancy loss rates in singleton pregnancies (from SET/DET) after transferring different types of embryos — from lowest to highest implantation potential. Day 3 embryos are less developed and generally less likely to implant, while blastocysts, especially good-quality day 5 ones, are more likely to implant and grow.
Their goal was to see whether DET increases the risk of miscarriage more when the embryos are of higher quality.
So what were the results?
- They started with day 3 cleavage-stage DET, which are earlier-stage and generally have a low potential of implantation. Here, DET showed a non-significant increase in the risk of miscarriage compared to SET (adjusted odds ratio [95% CI]: 1.18 [0.74-1.90], p= 0.46).
- Then they looked at mixed blastocyst DET, which involved a mix of good and lower quality blastocysts (and day 5 or 6) with a moderate to high potential of implantation. Here, DET also showed a non-significant increase in the risk of miscarriage compared to SET (adjusted odds ratio [95% CI]: 1.34 [0.96-1.87], p= 0.08).
- Finally, they focused on good quality day 5 blastocyst DET, which involved blastocysts with a high potential of implantation. Here, DET was significantly linked to a higher risk of miscarriage in singleton pregnancies (adjusted odds ratio [95% CI]: 1.55 [1.02-2.37], p= 0.04). This means miscarriage was significantly more likely—55% higher odds—in the DET group compared to SET.
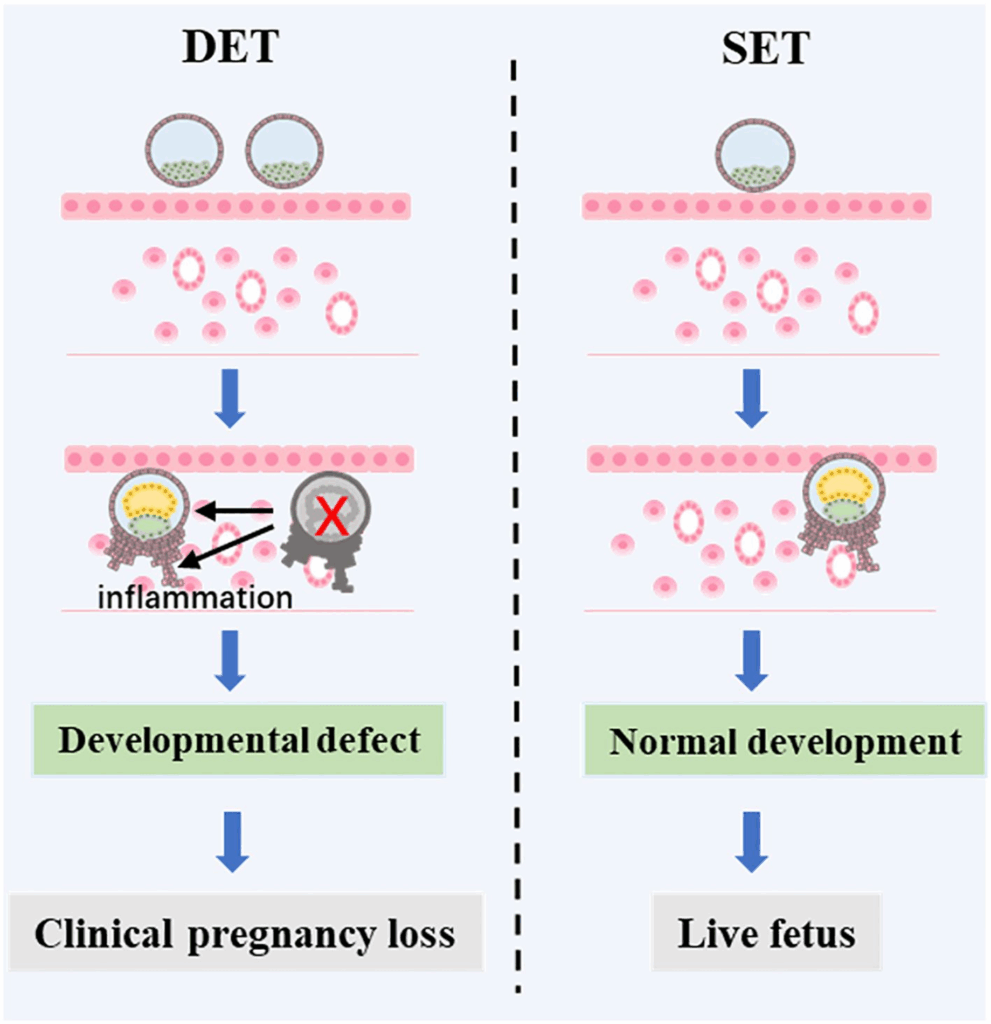
These results suggest that the better quality the embryos, the more risky it may be to transfer two instead of one. The authors believe that if one good quality embryo implants but then fails later, it could trigger inflammation in the uterus that harms the other embryo, leading to pregnancy loss.
So why did they only see an increase with good quality blastocysts?
- When two embryos are transferred, one may implant and then quickly fail to progress, either by arresting or degenerating (dying). This is more likely to happen with embryos that have a lower implantation potential like day 3 embryos or lower quality blastocysts (the “mixed blastocyst” group in this study). Because these embryos fail early, they may not trigger much of a maternal inflammatory response (they may never implant or become fully integrated into the uterine lining).
- If the embryo that fails is higher quality, as with good quality day 5 blastocysts, it may persist longer and become more integrated into the uterine lining before failing. This may trigger a stronger maternal inflammatory response that harms the implanted embryo, either by increasing the risk of miscarriage or by disrupting the uterine environment in ways that raise the chance of complications later in pregnancy.
The authors put together a figure to illustrate this:
Conclusions
This study found that DET increased the risk of miscarriage in singleton pregnancies only when both embryos were good quality day 5 blastocysts. There was no increased risk with lower quality blastocysts or with day 3 embryos.
Lower quality embryos tend to fail earlier and more quietly, without causing much disruption. Good quality blastocysts, on the other hand, are more likely to implant and stick around longer before failing, which could cause more inflammation and increase the risk of miscarriage or other complications for the remaining embryo.
This is supported by a number of other studies:
- A mouse study by Drews et al. (2020) investigated what happens when an embryo implants but fails to develop. They found that the embryo first undergoes apoptosis (self-destruction), and once its contents leak into the uterus, the mother’s body triggers an inflammatory response that clears the embryo through resorption — a process where the embryo is broken down and absorbed by the body. While this study wasn’t conducted in humans, it supports the idea that embryos that fail to develop after implantation can lead to an inflammatory response.
- Zhao et al. (2022) found that rising inflammation in the blood (of humans) from day 16 after embryo transfer was linked to miscarriage, while ongoing pregnancies showed a more balanced, anti-inflammatory response.
- A large study by Rodriguez-Wallberg et al. (2023) showed that singletons from DETs (compared to SETs) were at higher risk of adverse pregnancy outcomes like neonatal death, low birth weight and preterm birth. Similar results were also shown by Sutter (2006).
- Meja et al. (2020) compared cumulative live birth rates from a single retrieval cycle, showing that CLBR was higher for patients who had SET compared to DET, with SET births having a higher birthweight and reduced preterm births. Melado Vidales et al. (2023) included patients who had a euploid SET or DET, and found a higher pregnancy loss rate in DET patients (28.8% vs 22.8%).
Importantly, this study doesn’t directly show that both embryos implanted, that one was lost later, or that inflammation occurred.
This study adds to the evidence that a SET may be the better choice, particularly when higher quality embryos are available. While this study raises important questions about the risks of transferring two good quality embryos, it was conducted mostly in younger patients, where DET is already less common, and it’s less clear whether the same risks apply to older patients. Older patients were included, and the results held after adjusting for age, but a broader representation of older individuals would strengthen the conclusions (especially if euploids were used!). More research is needed!
Limitations include the retrospective, single-center design and baseline differences between groups: DET was more common in day 3 transfers and prior failed cycles, while SET was more common with good quality blastocysts and older patients. These differences may have introduced bias despite statistical adjustments.
To learn more about this topic, check out these related posts:
- Fetal reduction increases complications after double embryo transfer
- 2 embryos or 1? The risks of a double embryo transfer for women under 35
- ESHRE 2023 guidelines on the number of embryos to transfer
- How many embryos to transfer? 2021 ASRM recommendations
- Study examines transferring a good and poor quality embryo together
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 2 embryos or 1? The risks of a double embryo transfer for women under 35
2 embryos or 1? The risks of a double embryo transfer for women under 35
 Transferring a good and poor quality embryo together: a meta-analysis
Transferring a good and poor quality embryo together: a meta-analysis
 Researchers examine factors associated with preterm birth risk in IVF
Researchers examine factors associated with preterm birth risk in IVF
 ESHRE 2023 guidelines on the number of embryos to transfer
ESHRE 2023 guidelines on the number of embryos to transfer
 Study examines transferring a good and poor quality embryo together
Study examines transferring a good and poor quality embryo together
 How many embryos to transfer? 2021 ASRM recommendations
How many embryos to transfer? 2021 ASRM recommendations
 How many failed embryo transfers is too many?
How many failed embryo transfers is too many?
 Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes
Meta-analysis compares medicated and natural FET adverse pregnancy and birth outcomes