This post summarizes the 2025 ESHRE/ALPHA Istanbul consensus on egg and embryo assessment, offering patients a clear overview of how embryologists evaluate and rank eggs, zygotes, and embryos based on updated international guidelines.
Assessing eggs, zygotes, and embryos in the IVF lab is key for identifying which ones are most likely to result in a healthy pregnancy. However, the way this is done can vary widely between clinics.
To bring consistency to these assessments, two leading professional organizations in reproductive medicine — Alpha Scientists in Reproductive Medicine (ALPHA) and the European Society of Human Reproduction and Embryology (ESHRE) — developed the Istanbul Consensus in 2011. This consensus offered standard criteria and terminology for evaluating eggs, zygotes, and embryos.
Recently, these guidelines were updated to include new research and time-lapse imaging. A team of experts reviewed studies up to May 2024 and gathered input from 833 IVF professionals worldwide to put these guidelines together.
Below are the updated recommendations from ALPHA/ESHRE. This post offers a brief overview of most (but not all!) points along with their consensus, presented in a patient-friendly way. Please note that the full document is much more detailed and includes supporting research and references. You can access it here (open access).
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Table of Contents
Egg-related assessment
The following diagrams may be helpful for understanding some of the terminology in this section. For more information, you can check out my Complete guide to egg quality.


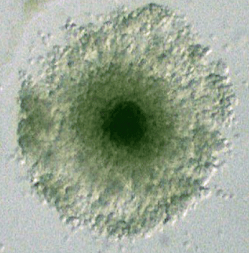
Cumulus oocyte complex (COC)
The COC includes the outer cumulus cells that surround the egg ater the egg is retrieved from the follicle. Studies suggest that very compact COCs and the presence of blood clots in the COC may reduce fertilization and pregnancy rates. ESHRE/ALPHA consensus: If most eggs show unusual COC characteristics, this should be noted.
Zona pellucida
The zona is the protective shell around the egg. While some studies link thick or dark zonas to poorer outcomes, the evidence is inconsistent. ESHRE/ALPHA consensus: Oocytes with different ZP appearances are OK for use.
Perivitelline space (PVS)
The PVS is the space between the egg and the zona. A large or granulated PVS has been linked to slightly lower fertilization, but findings are mixed. ESHRE/ALPHA consensus: Eggs with different PVS sizes or appearances are OK for use.
Polar body
Fragmented or large polar bodies show no strong link to poor outcomes, but very large polar bodies might suggest spindle issues. ESHRE/ALPHA consensus: Eggs with fragmented or large polar bodies can be used, but very large polar bodies should be noted.
Shape
Some oocytes are ovoid rather than perfectly round. Most studies show this doesn’t affect development or pregnancy. ESHRE/ALPHA consensus: Irregularly shaped oocytes are OK for use.
Egg size
Very small (<100 μm diameter) or large eggs (≥125 μm diameter) are rare and typically have low developmental potential, while giant oocytes (>180 μm diameter) are suspected to form from the fusion of primordial oocytes. ESHRE/ALPHA consensus: Giant oocytes should be excluded from use; very small or large oocytes may be used only if necessary and should be documented.
Vacuolization
Vacuoles are small fluid-filled spaces inside the egg’s cytoplasm. While associated with lower fertilization, they don’t predict poor embryo development. ESHRE/ALPHA consensus: Oocytes with vacuoles are OK for use; avoid injecting sperm into vacuoles during ICSI.
Refractile bodies
Refractile bodies are dense inclusions inside the egg’s cytoplasm. Larger refractile bodies (>5 μm) may lower fertilization rates, but don’t clearly affect embryo development. ESHRE/ALPHA consensus: Oocytes with refractile bodies, including large ones, are OK for use.
Smooth endoplasmic reticulum aggregates
Smooth endoplasmic reticulum aggregates are dense clusters in the egg’s cytoplasm. Newer studies show no major impact. ESHRE/ALPHA consensus: Oocytes with smooth endoplasmic reticulum aggregates can be used on a case-by-case basis.

Granularity
Cytoplasmic granularity refers to a non-uniform or rough appearance of the egg’s cytoplasm. Some studies suggest poor embryo outcomes while others find no impact. There’s no data on how granularity affects live births. ESHRE/ALPHA consensus: Oocytes with cytoplasmic granularity are OK for use.
Color
Some eggs appear darker or more translucent. There’s no clear link between color and embryo outcomes. ESHRE/ALPHA consensus: Oocytes with color variation are OK for use.
Immaturity
Immature eggs (M1 or GV) typically aren’t fertilized, but may be matured in the lab (rescue-IVM) in special cases. Their success rates are lower. ESHRE/ALPHA consensus: Rescue-IVM oocytes may be used in poor prognosis cases and should be documented.
Timing of fertilization and embryo development checks
Eggs fertilize and develop into embryos with a specific timing, and it’s important to observe key stages at standard times relative to insemination. Using a standardized time window for fertilization or embryo checks can help with benchmarking and tracking key performance indicators (KPIs), and is easiest when using time-lapse technology.
- Day 1 fertilization check (zygote): 16-17 hours post-insemination (ICSI or IVF). Checking later can miss pronuclei that already disappeared.
- Day 2 embryo check (cleavage stage): 43 hours (ICSI) or 45 hours (IVF) post-insemination (± 1 hour).
- Day 3 embryo check (cleavage stage): 63 hours (ICSI) or 65 hours (IVF) post-insemination (± 1 hour).
- Day 4 embryo check (morula stage): 93 hours (ICSI) or 95 hours (IVF) post-insemination (± 1 hour).
- Day 5 embryo check (blastocyst stage): 111 hours (ICSI) or 112 hours (IVF) post-insemination (± 1 hour).
Studies show that while IVF and ICSI embryos differ slightly in early timing, other patient and lab variables also influence development speed. Variations in timing can be normal and don’t necessarily predict worse outcomes.
ESHRE/ALPHA consensus: Standardize timing of embryo assessments relative to the time of insemination, reported as hours post-insemination, to ensure comparability across labs and studies.
Day 1 fertilization- or zygote-related assessment
Zygote size and pronuclei (PN) features
Zygote and pronuclear size, position, and behavior have been studied as potential indicators for embryo potential, but evidence is inconsistent and difficult to apply in practice. ESHRE/ALPHA consensus: Zygote size and PN details may be useful, but evidence is insufficient for their use in clinical practice.
Cytoplasmic halo
The halo is a clear zone seen in many zygotes shortly after fertilization. While its absence is linked to abnormal cleavage, studies suggest it does not impact pregnancy outcomes when embryos are transferred at the blastocyst stage. ESHRE/ALPHA consensus: A missing halo may be used to rank embryos at day 3, but should not be used to exclude embryos.
Nucleolar precursor bodies (NPBs)
NPBs are small structures inside pronuclei that relate to chromatin activity (chromatin is a form of compacted DNA). Studies are unclear on whether NPB clustering is helpful for predicting embryo development. ESHRE/ALPHA consensus: NPB patterns change too rapidly to be useful in static assessments.
Abnormal fertilization (0PN, 1PN, 3PN)
Zygotes that don’t show the typical two pronuclei (2PN) can still sometimes be viable. For example, embryos labeled 0PN, 1PN, or 2.1PN may still be diploid and capable of forming healthy blastocysts and live births, especially when confirmed by PGT.
ESHRE/ALPHA consensus: The presence of a second polar body, which emerges after successful fertilization, should be used alongside pronuclear assessment to confirm fertilization. Zygotes with a second polar body but no visible pronuclei should not be labeled “0PN” but instead as “PN not observed.” While 1PN and 2.1PN zygotes may be used cautiously, the use of 3PN zygotes is not recommended based on current data.
Check out my post on abnormal fertilization to learn more.
Day 2 or 3 cleavage stage embryo assessment
Cell numbers on day 2 and day 3
Embryos with 4 cells on day 2 and 8 cells on day 3 show the best chances for success. Too few or too many cells may signal problems, though some fast-growing embryos can still reach the blastocyst stage and have similar potential to day 3 embryos with 8 cells. ESHRE/ALPHA consensus: The best-performing early embryos have 4 cells on day 2 and 8 cells on day 3.
Fragmentation
Fragmentation refers to small pieces of cytoplasm breaking off from cells. Fragmentation is estimated by comparing it to cell size — for example, in a 4-cell embryo, 25% fragmentation means the fragments add up to the size of one cell. It can be hard to tell fragments apart from cells, but one study found that fragments smaller than 40 µm are not actual cells, suggesting this may be a useful cutoff for distinguishing between the two. More fragmentation is linked to lower live birth and implantation rates, but <10% fragmentation has little effect. ESHRE/ALPHA consensus: Embryos with >25% fragmentation have a low ranking; those with <10% fragmentation have a top ranking.
Cell size
At the 2-, 4-, and 8-cell stages, all cells should be about the same size because they’ve just finished dividing evenly, whereas at other times between divisions, cell sizes may naturally vary. Some studies define unequal cell size as having a cell that’s at least 25% smaller or larger than the average size of the other cells in a cleavage stage embryo. Unequal cell size has been linked to lower implantation rates and a higher risk of chromosomal abnormalities. ESHRE/ALPHA consensus: Cells should be evenly sized at key stages; uneven size may indicate reduced potential.
Multinucleation
Multinucleation (≥3 nuclei in a cell) is linked to poor outcomes and should be distinguished from binucleation (2 nuclei), which may not be harmful. ESHRE/ALPHA consensus: Multinucleation should be scored when using time-lapse, especially at the 4-cell stage.
Other morphological features
Features like spatial disorganization, membrane appearance, vacuoles, and cytoplasmic granularity may appear abnormal but don’t consistently affect embryo potential in studies.
Initiation of compaction
Compaction usually starts at the 8-cell stage or later; starting earlier may reduce blastocyst potential.
Ranking day 2 and day 3 embryos
- High priority: Embryos with 4 cells on day 2 or 8 cells on day 3 and <10% fragmentation are ranked highest for transfer or freezing.
- Intermediate priority: Those with more than 4 or 8 cells.
- Low priority: Embryos with fewer than 4 or 8 cells or >25% fragmentation are ranked lowest as they have been linked to poorer outcomes.
To read more about cleavage stage grading and success rates, check out my Complete guide to embryo grading and success rates.
Day 4 morula stage embryo assessment
Embryos that show full compaction or early cavitation by day 4 are more likely to form high-quality blastocysts and result in pregnancy. In contrast, partially compacted morulae with excessive fragmentation or excluded cells tend to have lower developmental potential, but may still be viable.
ESHRE/ALPHA consensus: Day-4 embryos with full compaction or early cavitation should be prioritized for transfer or freezing.
Day 5 blastocyst stage embryo assessment
Day of blastocyst formation
The day a blastocyst forms (day 5, 6, or 7) is closely linked to its success rate. Day 5 blastocysts tend to have higher implantation and live birth rates than those that form on day 6 or 7, though day 7 blastocysts can still lead to healthy births. This is true for untested and PGT tested (euploid) blastocysts. ESHRE/ALPHA consensus: Day of blastocyst formation is a key factor in determining which embryos are more likely to succeed and should be used in ranking.
Degree of expansion and ICM/TE grade
Blastocyst grading looks at how expanded the embryo is and how the inner cell mass (ICM) and trophectoderm (TE) appear. TE grade is most strongly linked with live birth, followed by expansion stage; ICM grade may matter less except when it’s very poor (grade C). ESHRE/ALPHA consensus: Expansion stage and TE grade are key for prioritizing blastocysts. Blastocysts with grade C ICM or TE could be OK for use.
Read more about this in my post Study evaluates which embryo grades predict IVF success.
Spontaneous collapse
As the blastocyst grows, sometimes it will spontaneously collapse, which is easiest to see with time-lapse imaging. Studies link spontaneous collapse to poorer quality and possibly lower euploidy rates, but its impact on pregnancy outcomes is still uncertain.
You can see a blastocyst expanding below, with multiple instances of spontaneous collapse, notably at 0:09 (Iwasawa et al. 2019, CC by 4.0):
This is different from an artificially collapsed blastocyst, where the embryologist intentionally collapses a blastocyst before freezing and re-expands after thawing. In contrast, spontaneous collapse occurs naturally without intervention.
Read more about embryo collapse/compaction in my post What is embryo compaction?
Cytoplasmic strings
These are thread-like structures connecting cells inside the blastocyst and are believed to aid communication between the ICM and TE. Blastocysts with strings tend to implant better, but it’s unclear if this should influence embryo selection alone.

Read more about this in my post Improved live birth rates in blastocysts with “cytoplasmic strings.”
Other morphological features
Blastocysts with two ICMs may increase the risk of monozygotic twinning and should not be transferred without clear patient counselling. The absence or degeneration of an ICM is linked to poor outcomes and such embryos should be considered non-viable and graded as ‘D’ rather than ‘C’.
To read more about blastocyst stage grading and success rates, check out my Complete guide to embryo grading and success rates.
Conclusions
The updated ALPHA/ESHRE recommendations provide evidence-based guidance for evaluating eggs, zygotes, and embryos in the IVF lab. While no system can perfectly predict success, these standards help labs make their assessments more consistently.
This consensus gives a good behind-the-scenes look at what happens in the IVF lab, and what leading IVF professionals consider to be the best practices when evaluating eggs, zygotes and embryos at different stages of development.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete Guide to Embryo Grading and Success Rates
Complete Guide to Embryo Grading and Success Rates
 Day 3 or Day 5 embryo transfer?
Day 3 or Day 5 embryo transfer?
 Increased risk factors with blastocyst transfer vs cleavage stage
Increased risk factors with blastocyst transfer vs cleavage stage
 Predicting how many day 3 embryos make it to blastocyst
Predicting how many day 3 embryos make it to blastocyst
 Predicting live birth rates, multiples based on 223,377 transfers
Predicting live birth rates, multiples based on 223,377 transfers
 Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation
Blastocyst and pregnancy rates of day 3 embryos based on cell number, fragmentation
 Transferring a good and poor quality embryo together: a meta-analysis
Transferring a good and poor quality embryo together: a meta-analysis
 Day 3 quality of a blastocyst is not linked to its chance of live birth
Day 3 quality of a blastocyst is not linked to its chance of live birth