A large 2025 study found that a thin lining (<7 mm) lowered live birth rates in medicated and modified natural FETs, but not in natural cycles, and overall endometrial thickness was not a strong standalone predictor of IVF success.
A thin endometrial lining is considered to be a barrier to IVF success, leading some clinics to cancel or delay embryo transfer if thickness is below a certain threshold.
But the evidence is mixed: some studies suggest outcomes drop below 6–8 mm, while others report no clear effect.
To address this, Genovese et al. (2025) carried out the largest study so far on single euploid blastocyst transfers after FET. By looking only at embryos that were chromosomally normal (euploid), they could remove much of the impact of egg quality and age, since the main reason age affects outcomes is the higher risk of abnormal embryos.
They also looked at how endometrial thickness influenced live birth rates in natural, modified natural and medicated FETs. To learn more about these different FET types, check out my post on Comparing frozen embryo transfer/FET protocols.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: International multicenter retrospective cohort study (2017–2022) across 25 IVF clinics in the USA, Spain, and UAE
- Participants: 30,676 FET cycles, each transferring a single euploid blastocyst from a patient’s own eggs
- FET cycle types: Medicated (78.6%), modified natural (19.0%), and natural (2.5%).
- Natural: Monitored spontaneous ovulation by measuring when progesterone increased past 1.5 ng/ml, transfer 5 days later with progesterone support (equivalent to day 6 of progesterone exposure). Note that many “true natural cycle” protocols rely on an LH surge, but definitions of the LH surge vary between clinics, which may explain why progesterone was used to monitor ovulation in this study.
- Modified natural: Natural cycle with hCG trigger when dominant follicle was 16-22 mm, transfer was also scheduled on the 6th day of progesterone exposure.
- Medicated: Estrogen to build lining then progesterone added when appropriate thickness was reached, and transfer was done on the 6th day of progesterone.
- Timing of endometrial thickness measurement: In natural and modified natural cycles, the lining was measured around the time ovulation occurred (either naturally or triggered with hCG), but the transfer itself was timed according to ovulation rather than the lining thickness. In medicated cycles, the lining was built up with estrogen and checked to ensure it had adequate thickness, with this measurement taken within 0–4 days before starting progesterone.
- Exclusions: Patients were excluded from this study if they had uterine anomalies, donor eggs, PGT-M, non-obstructive azoospermia, surgically retrieved sperm, double embryo transfer.
- Primary outcome: Live birth rate, delivery beyond 22 weeks
- Secondary outcomes: Effects of embryo quality, maternal age, BMI, and center-specific differences
How lining thickness relates to live birth after single euploid transfer
The researchers estimated the chance of live birth at different lining thicknesses, taking into account other factors like embryo quality, age, and BMI. The table below shows their predictions for natural, modified natural, and medicated cycles.
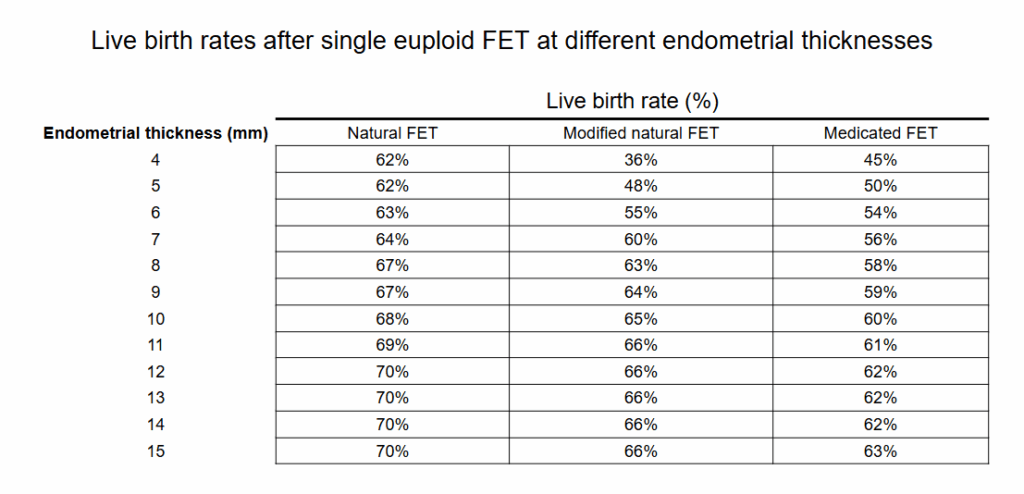
These results show that in medicated and modified natural cycles, success rates were lower when the lining measured under 7 mm, with live birth rates climbing as the lining grew thicker. By contrast, natural cycles were less affected by lining thickness — success rates stayed fairly steady across the range of measurements. Natural cycles were less affected by lining thickness, though only 2.5% of cases were natural cycles, so the small sample size may have limited the ability to see differences.
Even at very low thicknesses, some patients still achieved live births, though the chances may be lower in medicated and modified natural cycles. The authors reported 16 live births among women with an endometrial thickness under 5 mm, out of 42 single euploid transfers — a live birth rate of 38%.
The researchers also looked specifically at a 7 mm cutoff, which is commonly used in practice:
- Medicated FETs: Endometrial thickness <7 mm was linked with a 22% lower odds of live birth (adjusted odds ratio [95% CI]: 0.78 [0.70–0.87], p≤ 0.001).
- Modified natural FETs: Endometrial thickness <7 mm showed an even greater 41% reduction in odds of live birth (adjusted odds ratio [95% CI]: 0.59 [0.49–0.72], p< 0.001).
- Natural FETs: There was no statistically significant difference for the odds of live births in women with endometrial thickness <7 mm (adjusted odds ratio [95% CI]: 0.85 [0.58–1.25], p=0.41).
The researchers repeated their analysis in different ways (sensitivity analysis), such as only looking at the first transfer for each patient or making sure the lining measurement was taken very close to progesterone start. In all cases, the results were the same: live birth rates were lower when the lining was under 7 mm in medicated and modified natural cycles, but not in natural cycles. This suggests the findings are reliable.
Other factors linked to live birth
The researchers also examined how other factors influenced live birth by adjusting for everything together in one model. This showed which factors had an independent effect:
- FET protocol: Medicated transfers were associated with worse outcomes overall, with about a 31% lower odds of live birth compared with natural cycles. Modified natural cycles were not significantly different from natural cycles.
- BMI: Women with overweight had about an 8% lower odds of live birth compared with those in the normal BMI range. The effect was stronger for women with obesity: class I obesity was linked with a 13% lower odds, and class II obesity with a 22% lower odds.
- Embryo quality: ICM grade B embryos had about a 9% lower odds of live birth compared with grade A, while grade C embryos had a 52% lower odds. Similarly, trophectoderm grade B embryos had about a 7% lower odds compared with grade A, and grade C embryos about a 38% lower odds.
- Age: Maternal age did not affect outcomes until after 42 years, when women had about a 17% lower odds of live birth compared with those under 35.
This shows that while lining thickness matters, other factors like embryo quality, age, and BMI are often just as important, or more important, for predicting success
For comparison, as shown in the previous section, a lining under 7 mm was associated with a 22% lower odds of live birth in medicated cycles and a 41% lower odds in modified natural cycles, while natural cycles showed no significant difference.
When the researchers added lining thickness to models that already included factors like embryo quality, age, and BMI, it barely changed their ability to predict live birth. This shows that endometrial thickness on its own is not a strong predictor for live birth.
Conclusion
This study found that for medicated and modified natural FETs, live birth rates decreased when the thickness was <7 mm, but this wasn’t the case for natural FETs, which didn’t change across thicknesses.
The fact that there was no difference with natural FETs is interesting, so let’s look at it a bit more:
- The authors suggest that lining thickness may matter less for natural cycles because the endometrium develops in sync with the body’s own hormones.
- In this study, all natural cycles came from clinics in the UAE, where transfers were usually not canceled for thin linings (14.5% of cycles involved linings <7 mm in the UAE, vs 2.7% and 5.6% in the USA and Spain). This makes the UAE data more representative of the “true biology” of thin linings, especially in natural cycles. In the USA and Spain, by contrast, most thin-lining cycles were delayed or canceled, so the few patients who still had transfers with <7 mm linings likely represented a harder-to-treat group, which could help explain their lower success rates.
- Another factor, which wasn’t addressed by the authors of this study, is that there wasn’t a high number of natural FET cycles (only 2.5% of all cycles were natural, or 759 FETs), which could have influenced these results.
Overall, when they used a model that incorporated endometrial thickness along with many different factors, they found that endometrial thickness was not a strong predictor of live birth. Even in patients with “extremely thin” linings of <5 mm, there was a decent chance of live birth, and the authors write that “canceling cycles based on an arbitrary endometrial thickness threshold seems questionable.”
They also found higher live birth rates among patients who had a natural or modified natural FET compared to a medicated FET, which is consistent with recent studies.
Limitations include the retrospective design, variation in measurement timing, and possible unmeasured confounders (like the day of the euploid). Practice differences between centers — such as the UAE clinics more often proceeding with transfers in patients with thinner linings — may also have influenced the findings. Still, the large sample size and focus on single euploid transfers make this a very informative study on endometrial thickness and IVF outcomes.
Want to read more about endometrial thickness or different FET types?

The post discusses various frozen embryo transfer protocols, which includes a medicated FET, natural cycle FET (true natural/modified natural), and mild ovarian stimulated FET, along with their scheduling. In addition, it examines whether one FET protocol is superior to another, the relevance of the corpus luteum in medicated vs natural cycle FETs, and optimal progesterone levels. Read more.
A 2025 study found that live birth rates increased with endometrial thickness up to about 9 mm, after which they plateaued. Read more.
Researchers in a 2022 study compared the impact of endometrial thickness on pregnancy outcomes in fresh and frozen embryo transfer cycles. Read more.

A 2025 randomized controlled trial found that natural cycle FETs led to higher live birth rates and fewer miscarriages than medicated FETs in ovulatory women with a good prognosis. Read more.
Related studies
These additional studies were referenced by the authors of the paper and haven’t been covered on Remembryo. They may be helpful if you’re exploring this topic further. This section is available for paid subscribers.

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to embryo implantation and implantation failure
Complete guide to embryo implantation and implantation failure
 Endometrial thickness and pregnancy outcomes after 96,000 embryo transfers
Endometrial thickness and pregnancy outcomes after 96,000 embryo transfers
 Progesterone supplementation in true natural cycle FETs improves outcomes
Progesterone supplementation in true natural cycle FETs improves outcomes
 Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
Meta-analysis shows benefit of acupuncture on frozen embryo transfer outcomes
 Protected sex the night before frozen embryo transfer linked to improved outcomes
Protected sex the night before frozen embryo transfer linked to improved outcomes
 Study evaluates endometrial thickness and live birth rates in over 244,000 cycles
Study evaluates endometrial thickness and live birth rates in over 244,000 cycles
 Live birth rates higher with natural cycle FETs vs medicated FETs
Live birth rates higher with natural cycle FETs vs medicated FETs
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols