Researchers in a 2018 study found improved IVF and pregnancy outcomes in patients with no/low fertilization using artificial oocyte activation (AOA) to help activate the egg using the ionophore calcimycin or strontium chloride (SrCl2).
As the sperm nucleus enters the egg, it releases an enzyme called phospholipase C-zeta, which leads to the release of calcium ions (Ca2+). This surge of Ca2+ activates mitochondria in the egg to generate energy, which is needed for the egg to complete meiosis so the egg and sperm DNA can fuse to form the embryo’s DNA.
This process is called oocyte activation and is needed for successful fertilization.
In cases of total fertilization failure, or even in cases of low fertilization (<30% with ICSI), sometimes oocyte activation is blocked but can be corrected by artificial oocyte activation (AOA). There are different ways to induce oocyte activation, but using chemicals is the most common.
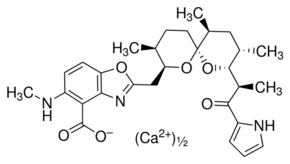
Calcimycin is an example of an ionophore. This is a molecule that has a special chemical structure that allows it to carry different ions, like the Ca2+ calcium ion, into the egg. This can artificially trigger oocyte activation. You can see the structure of the calcium ionophore calcimycin below:
Other chemicals can be used to release calcium ions like strontium chloride (SrCl2), which can bind to a special part of the egg cell called the endoplasmic reticulum to release calcium ions. So SrCl2 can also induce oocyte activation.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
A clinical trial by Fawzy et al. (2018) compared AOA using a calcium ionophore (calcimycin) and SrCl2. They compared these results to no AOA at all (ICSI alone).
All women were 18-40 with at least two previous ICSI cycles and low to no fertilization (0-30%), or with male factor infertility undergoing ICSI for the first time. These male-factor cycles had 100% abnormal sperm morphology with low counts (<10 million sperm/ml).
The clinical trial was conduced between 2015 and 2016, had 343 participants, and was divided into three groups:
- The calcimycin group (113 participants).
- The strontium chloride (SrCl2) group (115).
- The ICSI alone group (115).
They looked at multiple criteria between the groups.
In the SrCl2 group:
- Clinical pregnancy rates increased with SrCl2 compared to ICSI alone (49% vs 27%). This was statistically significant.
- Ongoing pregnancy rates increased (42% vs 23%).
- Live birth rates increased (40% vs 18%).
- Fertilization rates increased (85% vs 61%).
- Top quality Day 3 embryos increased (87% vs 57%).
- Blastocyst formation rates increased (62% vs 46%).
- Top quality blastocysts increased (41% vs 27%).
- Number of frozen blastocysts increased (44% vs 18%).
In the calcimycin group:
- Clinical pregnancy rates increased with calcimycin compared to ICSI alone (42% vs 27%). This was statistically significant.
- Ongoing pregnancy rates increased (36% vs 23%).
- Live birth rates increased (33% vs 18%).
- Fertilization rates increased (67% vs 61%).
- Blastocyst formation rates didn’t change(51% vs 47%).
- Top quality blastocysts didn’t change (27% vs 27%).
- Number of frozen blastocysts increased (29% vs 18%).
They also performed a subgroup analysis where they grouped their results based on couples who had done ICSI before but with low fertilization. For this group, SrCl2 was more effective than calcimycin. The reasoning for this is that calcimycin induces a single Ca2+ wave but not multiple waves in an oscillatory fashion like SrCl2 does. With normal sperm parameters, SrCl2 AOA may be more effective than calcimycin AOA.
Another subgroup analysis looked at male-factor infertility with abnormal sperm parameters. In this case, the egg may be activating normally, but the sperm is unable to trigger oocyte activation. With abnormal sperm parameters, calcimycin AOA may be more effective than SrCl2 AOA.
Although it’s convincing that calcimycin and SrCl2 both improve IVF outcomes, it’s not clear what the long term effects are. Because of this uncertainty, the authors state that their use in the general public is not recommended.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 Immature eggs matured in-lab for 2-6 h show acceptable IVF outcomes
Immature eggs matured in-lab for 2-6 h show acceptable IVF outcomes
 An Italian consensus on key performance indicators for assessing IVF clinics
An Italian consensus on key performance indicators for assessing IVF clinics
 First births using automated ICSI robot reported
First births using automated ICSI robot reported
 Egg freezing and thawing
Egg freezing and thawing
 No differences in IVF outcomes when using fresh or frozen donor eggs
No differences in IVF outcomes when using fresh or frozen donor eggs
 Early triggering with the “HIER” protocol may be a better approach for older women
Early triggering with the “HIER” protocol may be a better approach for older women
 Researchers develop tool to help predict fertilization failure
Researchers develop tool to help predict fertilization failure