In DOR patients, a 2025 study found that follicles measuring 15–17 mm at the time of egg retrieval were associated with the best outcomes, suggesting that optimal trigger timing in this group might occur earlier than standard thresholds used for normal responders.
In IVF, follicles grow to different sizes during stimulation, and monitoring their growth is necessary because follicle size is linked to egg maturity.
Current ESHRE guidelines recommend a broad trigger window of 16–22 mm for normal responders. However, this window may not apply to patients with diminished ovarian reserve (DOR), who often have fewer follicles and accelerated follicular development. This means that follicle size and timing of trigger might need to be assessed differently in DOR patients than in those with normal ovarian reserve.
A study by Naghshineh et al. (2025) wanted to determine the optimal follicle size for triggering in patients with DOR, to try to maximize oocyte maturity, fertilization, and embryo quality. Follicles were measured on the day of retrieval and aspirated individually so outcomes could be tracked back to the original follicle. According to the authors, follicles typically continue to grow by about 1–1.5 mm between trigger and retrieval.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Study type: Prospective study performed at a single academic fertility center in Iran between 2023 and 2024.
- Participants: 98 patients with DOR (POSEIDON groups 3 and 4) undergoing ICSI. In total there were 430 follicles: 155 follicles measured 11–14 mm, 168 measured 15–17 mm, and 107 measured ≥18 mm. The mean age was 36.0 years (range 22–44), with a mean AMH of 0.73 ng/mL. Patients with endometriosis, thyroid or prolactin disorders, chromosomal or genetic abnormalities, BMI >29 kg/m², or azoospermia in the male partner were excluded.
- Trigger and follicle measurement: Double trigger (GnRH agonist plus hCG) was administered when at least one follicle reached 17 mm, with the retrieval scheduled 36 h later. Individual follicles were measured and aspirated separately on the day of oocyte retrieval, with each oocyte and resulting embryo tracked back to its follicle of origin.
- Primary outcomes: Egg retrieval and oocyte maturity.
Follicle sizes 15–17 mm were associated with the best outcomes in DOR patients
After egg retrieval, each follicle was measured individually and linked to the oocyte and embryo that originated from it. In total, 430 follicles were aspirated and grouped based on their size on the day of retrieval (11-14 mm, 15-17 mm and ≥18 mm).
Egg retrieval rates (% of follicles with a retrieved egg) were highest for the 15-17 mm size (p= 0.001):
- 11–14 mm: 45.8%
- 15–17 mm: 88.1%
- ≥18 mm: 66.4%
Maturity rates were also highest for the 15-17 mm size (p= 0.001):
- 11–14 mm: 33.5%
- 15–17 mm: 83.3%
- ≥18 mm: 58.9%
Fertilization rates (per mature egg) were also highest for the 15-17 mm size (p= 0.001):
- 11–14 mm: 59.6%
- 15–17 mm: 97.1%
- ≥18 mm: 57.1%
Top quality embryo rates (day 3 embryos with good symmetry and ≤5% fragmentation) were also highest for the 15-17 mm size (p= 0.001):
- 11-14 mm: 38.7%
- 15–17 mm: 65.4%
- ≥18 mm: 58.3%
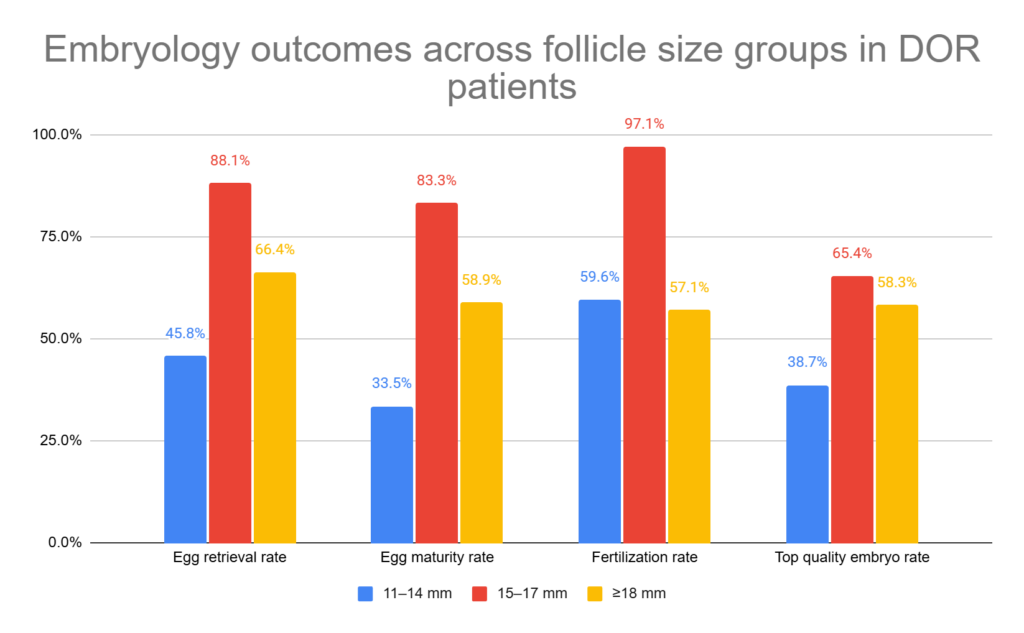
These results show that follicles in the 15–17 mm range were more likely to contain an oocyte, produce a mature oocyte, fertilize, and develop into a top-quality embryo compared with either smaller or larger follicles.
Subgroup analysis showed no significant differences between POSEIDON group 3 (<35 years) and group 4 (≥35 years), with the same optimal follicle size range of 15–17 mm observed in both age groups. This suggests that age had no impact on the follicle size associated with the best outcomes.
Characteristics associated with premature ovulation in DOR patients
Premature ovulation occurred in 13.3% of patients, and was associated with:
- Higher basal FSH (14.3 vs 7.1 mIU/ml)
- Lower AMH (0.43 vs 0.93 ng/ml)
- Higher LH on trigger day (20.27 vs 4.81 mIU/ml)
- Higher progesterone on trigger day (1.32 vs 0.68 ng/ml)
- Average size of leading follicle on trigger day: 18.6 mm
Conclusions
In this study, follicles measuring 15–17 mm at the time of egg retrieval were associated with the best outcomes for DOR patients, including higher egg retrieval, maturity, fertilization, and top-quality embryo rates. These findings were consistent across age groups.
One important limitation is that follicle size was measured on the day of egg retrieval rather than at the time of trigger. The authors note that follicles typically grew by about 1–1.5 mm between trigger and retrieval, so the optimal 15–17 mm size observed in this study likely corresponds to approximately 13.5–15.5 mm on the day of trigger. However, because trigger timing was not directly studied, further research is needed to confirm this, the authors write.
Studies in normal responders generally show that larger or mid-sized follicles (16-22 mm at trigger) are more likely to contain mature eggs and fertilize, although the exact “best” size differs between studies. In contrast, studies in poor responders and patients with DOR suggest that triggering at smaller follicle sizes (around 13–17 mm at trigger) may reduce premature ovulation without compromising egg maturity or embryo development. Together, this suggests that optimal trigger timing may be earlier and more narrow in DOR patients than in those with normal ovarian reserve.
In terms of the physiology behind this, the authors explain:
- In a normal cycle, follicles only respond to LH late in development, when LH receptors appear on granulosa cells. This allows the LH surge or trigger shot to complete egg maturation.
- In DOR, higher baseline FSH and lower AMH can cause LH receptors to appear earlier.
- This means follicles in DOR could reach maturity at smaller sizes.
- As a result, waiting for larger follicle sizes might not help, and triggering earlier at smaller sizes may be better in DOR patients.
Want to read more about follicle size and embryology outcomes?

What’s the ideal follicle size for IVF? Researchers in a 2022 study compared follicle size at the time of trigger and related it to rates for egg maturity, fertilization, good quality embryos and euploidy. They also examined the association between follicle size and age and BMI. Read more.

Researchers in a 2020 study compared IVF outcomes by follicle sizes, and found that larger follicles generally produced mature eggs that were more likely to develop into blastocysts. Read more.

Researchers in a 2023 study found that older women that are triggered earlier produce immature eggs that may be more competent than mature eggs after rescue IVM. Read more.
A 2024 meta-analysis combined the results of 12 studies comparing different IVF trigger shots, including hCG, GnRH agonist, and dual and double triggers. Triggers showed variable outcomes, highlighting the need for a personalized medicine approach. Read more.
Related studies
These additional studies were referenced by the authors of the paper and haven’t been covered on Remembryo. They may be helpful if you’re exploring this topic further. This section is available for paid subscribers.

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to egg quality
Complete guide to egg quality
 Study compares IVF outcomes by follicle size
Study compares IVF outcomes by follicle size
 Sleep quality and its impact on IVF outcomes
Sleep quality and its impact on IVF outcomes
 Follicle size linked to egg maturity, good quality embryo rate
Follicle size linked to egg maturity, good quality embryo rate
 Accelerated biological age linked to lower AMH, number of eggs retrieved
Accelerated biological age linked to lower AMH, number of eggs retrieved
 Early evidence suggests rapamycin may benefit aging eggs and improve IVF outcomes
Early evidence suggests rapamycin may benefit aging eggs and improve IVF outcomes
 Early triggering with the “HIER” protocol may be a better approach for older women
Early triggering with the “HIER” protocol may be a better approach for older women
 Meta-analysis ranks growth hormone, testosterone, other add-ons for low egg count
Meta-analysis ranks growth hormone, testosterone, other add-ons for low egg count