A 2025 randomized controlled trial found that patients with a low prognosis (expected to have <9 eggs retrieved) had higher live birth rates when doing a fresh transfer compared to frozen.
For low prognosis women, is a fresh or frozen transfer better?
Studies in women with normal or good prognosis have shown that the freeze-all strategy gives comparable or even higher live birth rates compared with fresh embryo transfer. However, it’s not clear what strategy is best for women with a low prognosis.
This post is a summary of a study by Wei et al. (2025), who performed a multi-center RCT that compared live birth rates in low prognosis patients who had a fresh or frozen transfer. Patients with a low prognosis had 9 or fewer eggs retrieved, AFC <5 or AMH <8.6 pmol/l (<1.2 ng/ml) based on the POSEIDON criteria.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
This section covers key details of how the study was performed, including patient characteristics, how they were treated, and other methods used. For those who aren’t interested in these details, and just want to see the results, you can go ahead and skip this part.
- This was a multicenter RCT that took place at nine IVF centers in China. The study was registered in 2021 and follow-up was complete by 2024.
- Inclusion: Patients undergoing their first or second IVF cycle, any age, with predicted 9 or fewer eggs retrieved/AFC <5/AMH <8.6 pmol/l (<1.2 ng/ml) based on the POSEIDON criteria.
- Exclusions: No premature increases in progesterone levels, no natural cycles for the egg retrieval, no PCOS, no uterine issues, no recurrent pregnancy loss patients.
- Patients were randomized on the day of egg retrieval to either have a fresh or frozen transfer, up to a year after randomization.
- Up to two good quality cleavage stage or blastocyst stage embryos were transferred (cleavage stage: 7–10 cells with low fragmentation; blastocyst: expansion ≥4 with ICM grade B or better). In the frozen group, non–day 5 blastocysts were cultured to day 6 or 7 (75% were transferred on day 5), while in the fresh group, embryos not reaching day 5 were frozen and later transferred (16 patients, included in the intention-to-treat analysis), per author correspondence.
- The primary outcomes was live birth after the first embryo transfer.
In terms of sample size, a total of 838 patients were randomized equally (419 per group) for the intention-to-treat analysis, with 387 in the fresh group and 331 in the frozen group meeting per protocol criteria (the drop was mainly due to protocol changes from fresh to frozen or vice versa). Additionally, 22 patients from the frozen group still didn’t have a transfer a year after randomization vs 2 in the fresh group. The study was powered at 80% to detect a 10% increase in live birth rate in the frozen transfer group.
This study allowed doctors and patients to decide on ovarian stimulation, embryo transfer numbers, and endometrial preparation for FET. While this approach may seem less controlled, it helps generalize results for broader applicability to the general public with the intention to treat analysis. The per protocol analysis will give a better idea of what happens when the patient sticks to the group they were assigned.
Baseline characteristics were similar, with an average age of about 34. The fresh group had more single day 5 transfers and fewer double day 3 transfers. In the frozen group, transfers were 20.5% one day 3, 49.6% two day 3, 29.3% one blastocyst, and 0.6% two blastocysts, versus 21.8%, 58.8%, 18.9%, and 0.5% in the fresh group.
Pregnancy outcomes for first fresh or frozen transfer
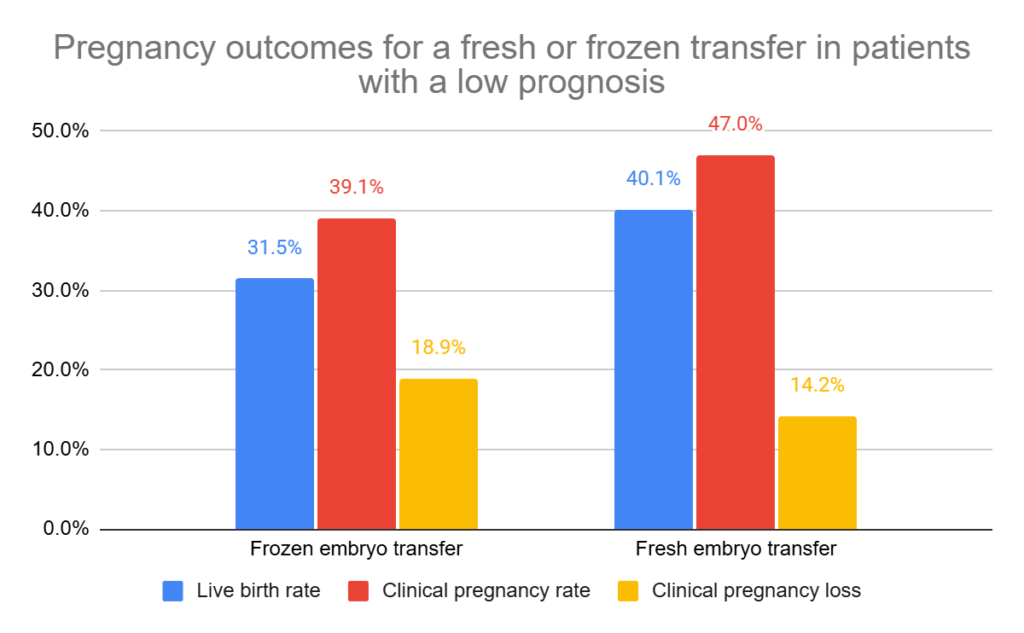
This study found that patients had a lower live birth rate with a first frozen transfer vs a first fresh transfer from a single ovarian stimulation cycle (31.5% vs 40.1%, relative ratio [95% CI]: 0.79 [0.65-0.94], p= 0.009). This was for the intention to treat analysis, but they also found a similar difference in the per protocol analysis (31.4% vs 40.6%, relative ratio [95% CI]: 0.77 [0.63-0.95]).
See my glossary page for intention to treat and per protocol if you’re unsure of these terms.
Twin live birth rates were lower in patients having a frozen transfer vs fresh (4.8% vs 9.1%, p= 0.01). This is likely because there were fewer double day 3 transfers in the frozen group compared to fresh, as described in the study details section above.
There was also a lower clinical pregnancy rate with a first frozen transfer. There were no statistical differences in the clinical pregnancy loss rate, or in the total pregnancy loss rate (including biochemical, clinical, first and second trimester losses).
They also measured the cumulative live birth rate, which included all transfers up to a year after their single ovarian stimulation cycle, with a lower CLBR for frozen transfers vs fresh (44.2% vs 51.3%, relative ratio [95% CI]: 0.86 [0.75-0.99], p= 0.04).
This data was for the intention to treat analysis, but the per protocol analysis was similar.
No adverse pregnancy outcomes with fresh vs frozen
They also looked at adverse pregnancy outcomes between the fresh and frozen groups, finding NO difference in:
- Ectopic pregnancy among biochemical pregnancies
- Gestational diabetes among clinical pregnancies
- Gestational hypertension among clinical pregnancies
- Pre-eclampsia among clinical pregnancies
- Placenta previa among clinical pregnancies
- Premature rupture of membranes among clinical pregnancies
- Stillbirth among deliveries
- Postpartum haemorrhage among deliveries
- Preterm delivery among deliveries
- Large for gestational age among live newborns
- Small for gestational age among live newborns
- Neonatal jaundice among live newborns
- Neonatal infection among live newborns
- Neonatal hospitalisation >3 days among live newborns
- Neonatal death among live newborns
- Congenital anomalies among live newborns
Conclusions
This study found that patients had a lower live birth rate for frozen vs fresh transfers. There were also lower clinical pregnancy rates, but no change in pregnancy loss rates.
This is different from the results of studies done in good prognosis patients, which often find no difference or a lower chance with fresh transfers. I’ll reference these studies below, but I did summarize one of these studies in my post Fresh or frozen embryo transfer? Results of the E-Freeze clinical trial.
The authors explain that good prognosis patients have higher hormone levels that could have a negative effect on the endometrium during a fresh transfer, making them potentially less effective.
On the other hand, the authors explain, patients with a low prognosis have lower levels of these hormones so the negative effect on the endometrium might be less. Instead, any negative effects from freezing the embryo might be amplified, causing lower success rates with frozen transfers.
Most studies find that freezing embryos is safe, but there are some that find otherwise (ie. multiple freeze-thaws for biopsied embryos seems to have a negative effect, based on this meta-analysis). It’s also possible that different patient groups experience different outcomes.
Anyways, that’s their hypothesis to explain the results of their study. Whether it’s true or not will require more studies.
The major limitation of this study, as discussed by the authors, was that the trial allowed for patient and doctor preferences. This resulted in more single blastocyst transfers in the frozen group and more double cleavage-stage transfers in the fresh group, which increased twin live birth rates in the fresh group. These differences could have accounted for the difference in live birth rates. The authors state that more standardized trials are needed to confirm the findings (ie. with only single blastocyst transfers).
While this might be seen as a negative thing, it’s important to recognize that this study design helps to generalize the results for a wider range of clinical practices.
Another concern is the high number of protocol deviations in the frozen group—88 patients deviated (62 switched to a fresh protocol and 22 did not have a transfer within a year)—compared with only 32 deviations in the fresh group (30 switched and 2 did not transfer within a year). The authors performed an “optimistic estimation” by assuming that all patients who did not transfer within a year eventually achieved a live birth, which is an unlikely scenario, but they found no statistical difference between fresh and frozen transfers in this case (41% vs 37%). The per protocol analysis excluded these patients entirely, and still showed that fresh transfers performed better.
Based on this, having a fresh transfer is a good idea for patients with a low prognosis. For patients who can’t, because of progesterone levels for example, it’s a better idea to freeze anyway since this can lower live birth rates. Patients with higher progesterone levels were specifically excluded from this study. For patients who are banking embryos, or doing PGT, the authors note that there needs to be more studies done for those with a low prognosis.
Related studies
To learn more about this topic, you can check out a number of studies referenced in this study below (7 links):

Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Risk of poor ovarian response with repeat IVF cycles
Risk of poor ovarian response with repeat IVF cycles
 Impact of delayed treatment on IVF outcomes
Impact of delayed treatment on IVF outcomes
 Comparing frozen embryo transfer/FET protocols
Comparing frozen embryo transfer/FET protocols
 Prolonged frozen embryo storage may result in lower success
Prolonged frozen embryo storage may result in lower success
 Study finds poor ovarian responders have no further live births after 4 cycles
Study finds poor ovarian responders have no further live births after 4 cycles
 Comparing IVF outcomes from cycles with low AMH
Comparing IVF outcomes from cycles with low AMH
 Prolonged embryo storage >6 years may reduce pregnancy, live birth rates
Prolonged embryo storage >6 years may reduce pregnancy, live birth rates
 Examining live birth rates in IVF cycles with 5 or less follicles
Examining live birth rates in IVF cycles with 5 or less follicles