Researchers in a 2023 study found that increasing female BMI resulted in decreased pregnancy and live birth rates after a single euploid transfer, while pregnancy loss rates increased. This effect was reduced in cases of male factor infertility only, suggesting that weight itself may not be responsible.
This study compared pregnancy outcomes of 55,564 women with increasing BMI following the transfer of a single euploid embryo. Data was collected using the Society for Assisted Reproductive Technology (SART) database between 2016-2019. SART is an IVF registry for the US and collects data from most clinics in the country.
🔗 Original studies are referenced in this post or within the linked Remembryo posts.
💡 Reminder: Terms underlined with a dotted black line are linked to glossary entries. Clicking these does not count toward your paywall limit.
Study details
- Cycles were PGT (PGT-A, PGT-SR, PGT-M, PGT-HLA) and involved the patient’s eggs (no donor eggs). A single euploid was transferred and this was the first transfer. Different frozen embryo transfer protocols were used and not recorded in the SART data.
- Exclusions: Missing cycle data or data that was obviously incorrect, recurrent pregnancy loss cycles, uterine factor infertility cycles.
- A pregnancy loss was any clinical pregnancy that was lost before 24 weeks (therapeutic and spontaneous losses were not distinguished in the SART data).
The 55,564 patients were grouped based on their BMI (<18.5, 18.5-24.9, 25-29.9, 30-34.9, 35-39.9, 40-44.9, 45-49.9, >50). The age of women varied from 34.3 ± 4.4 to 36.7 ± 4.2. Multiple logistic regression was used to statistically adjust, or control, for differences between the groups (age at transfer, smoking status, race, reason for PGT, endometrial thickness, previous pregnancy loss).
In addition to looking at the outcomes based on the different BMI categories, the researchers also performed a continuous analysis. This involves treating BMI as a continuous numerical value instead of dividing it into BMI categories. This allowed them to see how smaller changes in BMI can contribute to outcomes.
Worsened pregnancy outcomes with increasing BMI following single euploid transfer
You can see the results from the 55,564 single euploid transfers below.
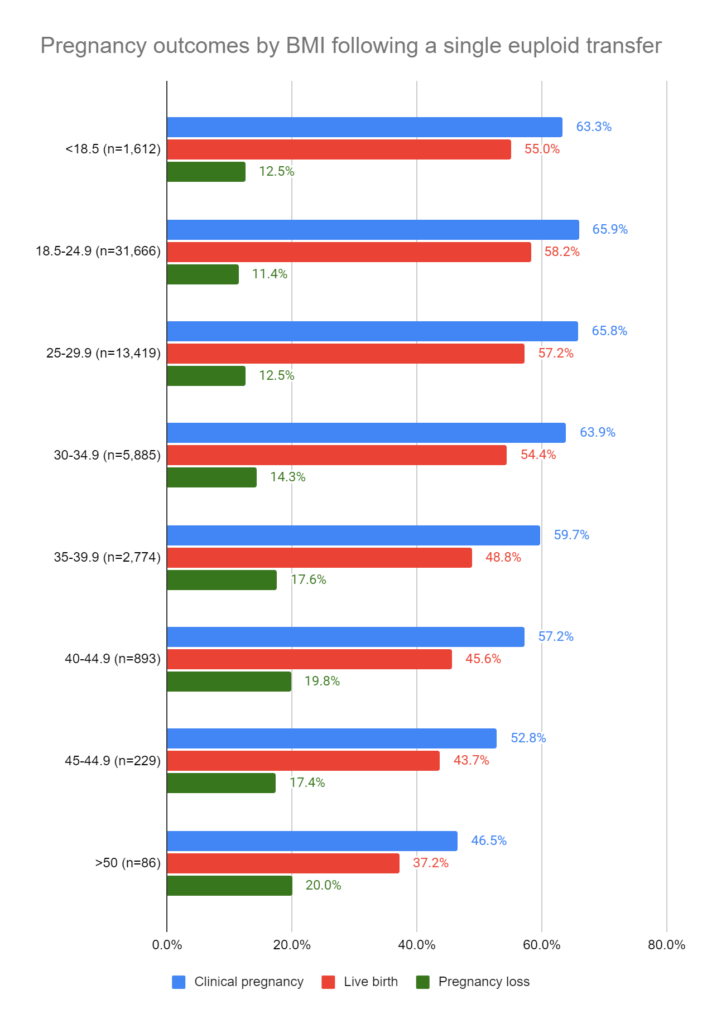
Because of the large sample size, most of this was statistically significant (by odds ratios). I’ll make some comments on this below.
For clinical pregnancy and live birth, compared to women with a BMI of 18.5-24.9, there was NO difference in the BMI 25-29.9 group, but there were differences for every other group.
For pregnancy loss, compared to women with a BMI of 18.5-24.9, there was NO difference for women with a BMI of <18.5, 45-49.9 and >50.
For their continuous analysis, for every increase in BMI by 1, there was a decrease in the odds of clinical pregnancy and live birth by 2%, and an increase in the odds of pregnancy loss by 2%.
Subgroup analysis on women with PCOS shows a similar trend with increasing BMI
Weight gain is a common symptom of PCOS, so they did a subgroup analysis looking at women with only PCOS.
For live birth rates, compared to the BMI 18.5-24.9 group (with a birth rate of 56.7%), there were no statistically significant differences between BMI <18.5 and 34.9. There was a lower live birth rate with BMI 35-39.9 (44.7%) and BMI 40-44.9 (45.0%), while above BMI 45 there weren’t any differences (although the sample size was small).
The same was mostly true for pregnancy losses (BMI 18.5-24.9 had a rate of 13.2%, which only showed a statistically significant difference with BMI 35-39.9, at a rate of 21.8%; larger BMIs had a small sample size).
For their continuous analysis, for every increase in BMI by 1, there was a decrease in the odds for clinical pregnancy by 1%, by 2% for live birth, and an increase in the odds of pregnancy loss by 2%.
Subgroup analysis on cycles with male factor show reduced impact of BMI
They also did a subgroup analysis on women with male factor infertility only.
For live birth rates, compared to the BMI 18.5-24.9 group (with a birth rate of 60.2%), there were no statistically significant differences between BMI <18.5 and 40. There was a lower live birth rate with BMI 40-44.9 (48.0%), but above BMI 45 there weren’t any differences (although the sample size was small).
Pregnancy losses were similar (BMI 18.5-24.9 had a rate of 10.4%, which only showed a statistically significant difference with BMI 35-39.9, at a rate of 14.1%; larger BMIs had a small sample size).
For their continuous analysis, for every increase in BMI by 1, there were no changes in clinical pregnancy, live birth or pregnancy loss.
This suggests that pregnancy outcomes aren’t affected as much with increasing female BMI with a male factor diagnosis.
Conclusions
As female BMI increased, this study found an overall decrease in pregnancy and live birth rates, with an increase in pregnancy loss rates.
Women with PCOS only showed a similar trend to the overall results, with a decrease in pregnancy and live birth rates with female BMI, while pregnancy loss rates increased.
Despite this, euploid transfers in obese women still resulted in high chances of live birth, even with the largest BMI category. Because of this, the authors stress that IVF is a viable treatment for obese women with infertility, with proper counseling.
Interestingly, cycles involving male factor only diagnoses showed a reduced impact of female BMI on pregnancy outcomes, so the decreases we’re seeing may only apply to infertile women. This suggests that weight itself may not influence pregnancy outcomes, unless it’s combined with infertility.
There are limitations with using BMI as a marker for body fat. BMI is a measure of excess weight, which doesn’t necessarily imply a high level of body fat, and doesn’t account for factors like age, sex, and muscle mass. It’s possible that some women with a higher BMI don’t have much body fat at all. To better understand the impact of body fat on pregnancy outcomes, more studies are needed using measurement methods that are more accurate.
Reference

About Embryoman
Embryoman (Sean Lauber) is a former embryologist and the founder of Remembryo, an IVF research and fertility education website. After working in an IVF lab in the US, he returned to Canada and now focuses on making fertility research more accessible. He holds a Master’s in Immunology and launched Remembryo in 2018 to help patients and professionals make sense of IVF research. Sean shares weekly study updates on Facebook, Instagram, and Reddit regularly. He also answers questions on Reddit or in his private Facebook group.
Related posts:
 Complete guide to egg quality
Complete guide to egg quality
 Why do embryos in IVF fail to implant or miscarry?
Why do embryos in IVF fail to implant or miscarry?
 Impact of supplements on live birth and pregnancy rates in women: a meta-analysis
Impact of supplements on live birth and pregnancy rates in women: a meta-analysis
 Rising levels of chlormequat, an agricultural chemical linked to infertility, in grain products
Rising levels of chlormequat, an agricultural chemical linked to infertility, in grain products
 The role of popular diets on fertility and IVF outcomes
The role of popular diets on fertility and IVF outcomes
 Comprehensive review combines research on use of supplements for female infertility
Comprehensive review combines research on use of supplements for female infertility
 Meta-analysis combines results of 16 studies on DHEA supplementation before IVF
Meta-analysis combines results of 16 studies on DHEA supplementation before IVF
 Silent insulin resistance is common, linked to lower IVF success rates
Silent insulin resistance is common, linked to lower IVF success rates